

100 consecutive minimally invasive Heller myotomies: lessons learned
- PMID: 11981208
- PMCID: PMC1422488
- DOI: 10.1097/00000658-200205000-00004
100 consecutive minimally invasive Heller myotomies: lessons learned
Abstract
Objective: To evaluate the authors' first 100 patients treated for achalasia by a minimally invasive approach.
Methods: Between November 1992 and February 2001, the authors performed 95 laparoscopic and 5 thoracoscopic Heller myotomies in 100 patients (age 49.5 +/- 1.5 years) with manometrically confirmed achalasia. Before presentation, 51 patients had previous dilation, 23 had been treated with botulinum toxin (Botox), and 4 had undergone prior myotomy. Laparoscopic myotomy was performed by incising the distal 4 to 6 cm of esophageal musculature and extended 1 to 2 cm onto the cardia under endoscopic guidance. Fifteen patients underwent antireflux procedures.
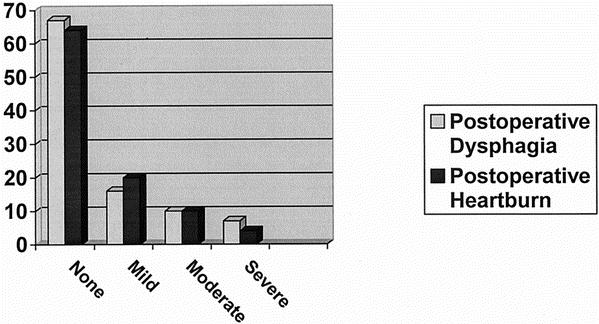
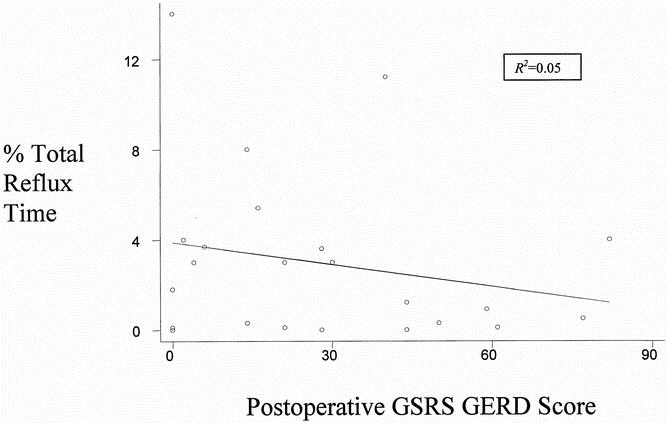
Results: There were eight intraoperative perforations and only four conversions to open surgery. Follow-up is 10.8 +/- 1 months; 75% of the patients have been followed up for at least 14 months. Outcomes assessed by patient questionnaires revealed satisfactory relief of dysphagia in 93 patients and "poor" relief in 7 patients. Postoperative heartburn symptoms were reported as "moderate to severe" in 14 patients and "none or mild" in 86 patients. Fourteen patients required postoperative procedures for continued symptoms of dysphagia after myotomy. Esophageal manometry studies revealed a decrease in lower esophageal sphincter pressure (LESP) from 37 +/- 1 mm Hg to 14 +/- 1 mm Hg. Patients with a decrease in LESP of more than 18 mm Hg and whose absolute postoperative LESP was 18 or less were more likely to have relief of dysphagia after surgery. Thirty-one patients who underwent Heller alone were studied with a 24-hour esophageal pH probe and had a median Johnson-DeMeester score of 10 (normal <22.0). Mean esophageal acid exposure time was 3 +/- 0.6% (normal 4.2%). Symptoms did not correlate with esophageal acid exposure.
Conclusions: The results after minimally invasive treatment for achalasia are equivalent to historical outcomes with open techniques. Satisfactory outcomes occurred in 93% of patients. Patients whose postoperative LESP was less than 18 mm Hg reported the fewest symptoms. After myotomy, patients rarely have abnormal esophageal acid exposure, and the addition of an antireflux procedure is not required.
Figures
References
-
- Heller E. Extramukose kerkioplastic beim chronischen Kardiospasmus mit Dilatation des Oesophagus Mitt Grenzgeb. Med Chir 1914; 27: 141–149.
-
- Ellis FH, Jr., Olsen AM, Holman CB, et al. Surgical treatment of cardiospasm (achalasia of the esophagus): consideration of aspects of esophagomyotomy. JAMA 1958; 166: 29. - PubMed
-
- Shimi S, Nathanson LK, Cushieri A. Laparoscopic cardiomyotomy for achalasia. J R Coll Surg Edinb 1991; 36: 152–154. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
