

Three hundred consecutive emergent celiotomies in general surgery patients: influence of advanced diagnostic imaging techniques and procedures on diagnosis
- PMID: 11981214
- PMCID: PMC1422494
- DOI: 10.1097/00000658-200205000-00010
Three hundred consecutive emergent celiotomies in general surgery patients: influence of advanced diagnostic imaging techniques and procedures on diagnosis
Abstract
Objectives: To assess the utility of advanced tests performed before surgery on patients who needed emergent abdominal operations, and to assess the outcomes of these patients relative to their diagnoses.
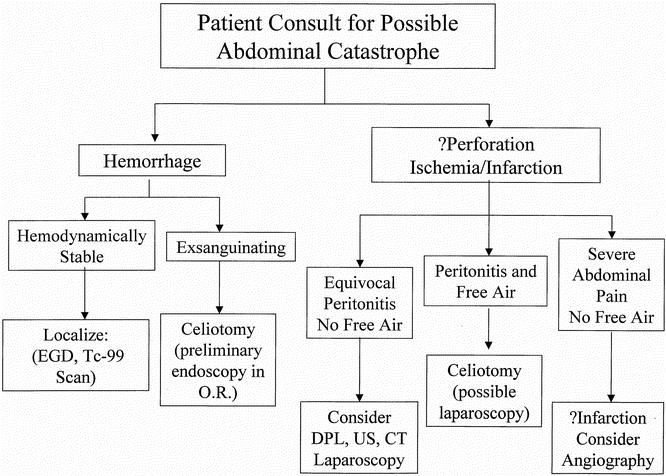
Summary background data: Patients with a potential abdominal catastrophe may have various presentations, contributing to the difficulty of the decision about whether an operation is indicated. Advanced tests can be valuable, but the use of these adjuncts should be appropriate to the clinical status of the patient so that treatment is not delayed. The role of these tools in the evaluation of the patient who may need an emergent abdominal operation is less well defined.
Methods: Data were reviewed on adult patients undergoing emergent abdominal operations. Entrance criteria included patients who had an emergent abdominal operation, defined as one performed for presumed gastrointestinal perforation, infarction, or hemorrhage within 6 hours of admission or surgical consultation. Advanced tests were those that were time-consuming or invasive or required scheduling with other departments so that the risk/benefit ratio of these tests could be questioned. A useful test was one that provided information that contributed to a change in the patient's management.
Results: During a 5-year period, 300 consecutive adult patients (158 perforations, 66 hemorrhage, 53 ischemia/infarction, and 23 "other") underwent emergent nontrauma celiotomies. Overall, the death rate was 20%. Advanced preoperative tests were performed in 135 (45%) of the 300 patients, and 40 of these patients had delayed treatments. Preoperative localization of bleeding sites was accomplished in 77% of patients with upper gastrointestinal bleeding and 86% of patients with lower gastrointestinal bleeding.
Conclusions: Most patients in need of emergent abdominal operations should not undergo advanced tests. The primary role of advanced tests in these patients is in the localization of a bleeding site. With the exception of patients who present with hemorrhage, advanced tests frequently cause a delay in treatment.
Figures


References
-
- Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA 1961; 178: 261. - PubMed
-
- Cohen FS, Sohn N. Lower gastrointestinal bleeding. In: Cameron JL. Current surgical therapy, 7th ed. St. Louis: Mosby; 2001: 322–327.
-
- Rantis PC, Harford FJ, Wagner RH, Henkin RE. Technetium-labelled red blood cell scintigraphy. Is it useful in acute lower gastrointestinal bleeding? Int J Colorectal Dis 1995; 10: 210–215. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
