

Klippel-Feil syndrome - the risk of cervical spinal cord injury: a case report
- PMID: 11985781
- PMCID: PMC107839
- DOI: 10.1186/1471-2296-3-6
Klippel-Feil syndrome - the risk of cervical spinal cord injury: a case report
Abstract
Background: Klippel-Feil syndrome is defined as congenital fusion of two or more cervical vertebrae and is believed to result from faulty segmentation along the embryo's developing axis during weeks 3-8 of gestation. Persons with Klippel-Feil syndrome and cervical stenosis may be at increased risk for spinal cord injury after minor trauma as a result of hypermobility of the various cervical segments. Persons with Klippel-Feil Syndrome often have congenital anomalies of the urinary tract as well.
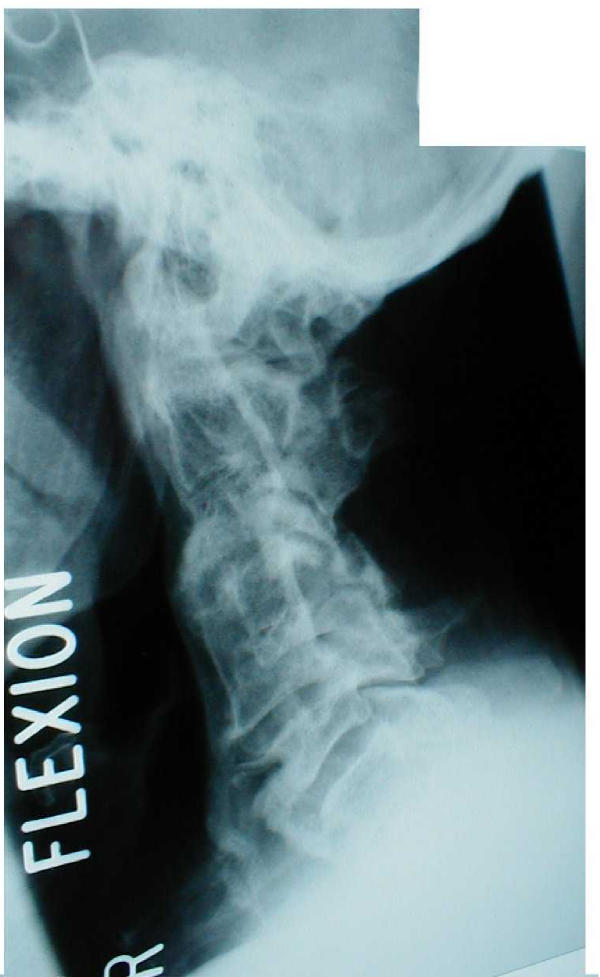
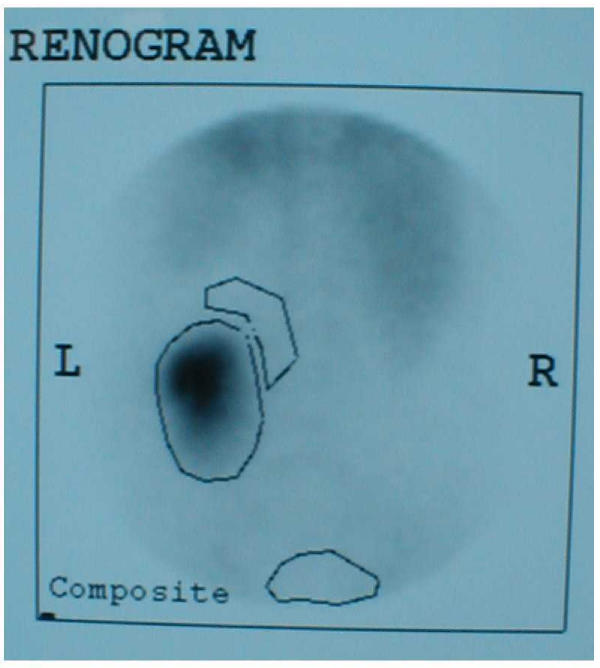
Case presentation: A 51-year male developed incomplete tetraplegia in 1997 when he slipped and fell backwards hitting his head on the floor. X-rays of cervical spine showed fusion at two levels: C2 and C3 vertebrae, and C4 and C5 vertebrae. Intravenous urography (IVU) revealed no kidneys in the renal fossa on both sides, but the presence of crossed, fused renal ectopia in the left ilio-lumbar region. This patient had a similar cervical spinal cord injury about 15 years ago, when he developed transient numbness and paresis of the lower limbs following a fall.
Discussion and conclusion: 1) Persons with Klippel-Feil syndrome should be made aware of the increased risk of sustaining transient neurologic deterioration after minor trauma if there is associated radiographic evidence of spinal stenosis.2) Patients with Klippel-Feil syndrome often have congenital anomalies of the urinary tract. Our patient had crossed, fused, ectopia of kidney.3) When patients with Klippel-Feil syndrome sustain tetraplegia they have increased chances of developing urinary tract calculi. Treatment of kidney stones may pose a challenge because of associated renal anomalies.4) Health professionals caring for cervical spinal cord injury patients with Klippel-Feil syndrome and renal anomalies should place emphasis on prevention of kidney stones. A large fluid intake is recommended for these patients, as a high intake of fluids is still the most powerful and certainly the most economical means of prevention of nephrolithiasis.
Figures




References
-
- Strax TE, Baran E. Traumatic quadriplegia associated with Klippel-Feil syndrome: discussion and case reports. Arch Phys Med Rehabil. 1975;56:363–365. - PubMed
-
- Karasick D, Schweitzer ME, Vaccaro AR. The traumatized cervical spine in Klippel-Feil syndrome: imaging features. A JR Am J Roentgenol. 1998;170:85–88. - PubMed
-
- Elster AD. Quadriplegia after minor trauma in the Klippel-Feil syndrome: A case report and review of the literature. J Bone Joint Surg Am. 1984;66:1473–1474. - PubMed
-
- Vaidyanathan S, Glass CA, Soni BM, Bingley J, Singh G, Watt JWH, Sett P. Doctor-Patient Communication: Do people with spinal cord injury wish to receive written information about their medical condition from the physicians after an outpatient visit or after a readmission in the spinal unit? Spinal Cord. 2001;39:650–653. doi: 10.1038/sj.sc.3101224. - DOI - PubMed
-
- Moore WB, Matthews TJ, Rabinowitz R. Genitourinary anomalies associated with Klippel-Feil syndrome. J Bone Joint Surg Am. 1975;57:355–357. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
