

Vitamin A levels and immunity in humans
- PMID: 11986269
- PMCID: PMC119985
- DOI: 10.1128/cdli.9.3.616-621.2002
Vitamin A levels and immunity in humans
Abstract
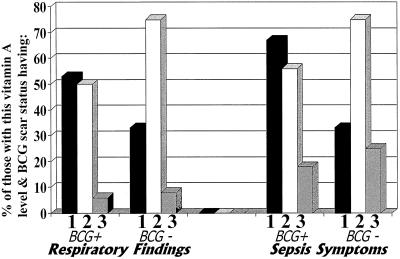
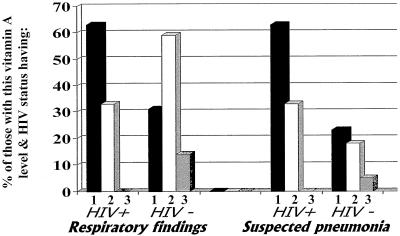
In animal studies, vitamin A deficiency induces a shift from type 2 (humoral) to type 1 (cellular) cytokines; there are no similar data for humans. Control of human immunodeficiency virus (HIV) and Mycobacterium tuberculosis infections requires type 1 cytokine (cellular) immunity. These infections and vitamin A deficiency are highly prevalent in Africa. We therefore examined the interactions among serum vitamin A levels, immune parameters, HIV infection status, Mycobacterium bovis BCG vaccine scarring (as an indicator of a type 1 cytokine profile), and clinical findings for 70 hospitalized children in Malawi, Africa. Directly conjugated monoclonal antibodies and flow cytometry were used to assess cell-specific cytokine production by peripheral blood monocytes and lymphocyte subpopulations. The statistical techniques employed included nonparametric statistics and logistic regression analyses. Thirty percent of the participants had severe vitamin A deficiency (<10 microg/dl), 34% had moderate deficiency (10 to <20 microg/dl), and 36% had normal levels (> or = 20 microg/dl). Vitamin A levels were lower for HIV-positive than for HIV-negative children (median, 10 and 17 microg/dl, respectively). Vitamin A-deficient children (<20 microg/dl) were more likely than non-vitamin A-deficient children to have higher proportions of natural killer (NK) cells (median, 8.3 and 5.2%, respectively) and lower ratios of interleukin-10-producing monocytes to tumor necrosis factor alpha-producing monocytes after induction (median, 1.0 and 2.3, respectively). Vitamin A-deficient children were also more likely than non-vitamin A-deficient children to exhibit respiratory symptoms (47% versus 12%) and visible BCG vaccine scars (83% versus 48%), which are indicative of a type 1 response to vaccination. Vitamin A status did not vary with gender, age, incidence of malaria parasitemia, blood culture positivity, or rates of mortality (6% of vitamin A-deficient children died versus 20% of non-vitamin A-deficient children). Lower vitamin A levels were associated with a relative type 1 cytokine dominance and proportionately more NK cells, both of which may be somewhat beneficial to persons who are exposed to HIV, M. tuberculosis, or other type 1 pathogens.
Figures
References
-
- Aukrust, P., F. Müller, T. Ueland, A. M. Svardal, R. K. Berge, and S. S. Frøland. 2000. Decreased vitamin A levels in common variable immunodeficiency: vitamin A supplementation in vivo enhances immunoglobulin production and downregulates inflammatory responses. Eur. J. Clin. Investig. 30:252-259. - PubMed
-
- Bloem, M. W., M. Wedel, R. J. Egger, A. J. Speek, J. Schrijver, S. Saowakontha, and W. H. P. Schreurs. 1990. Mild vitamin A deficiency and risk of respiratory tract diseases and diarrhea in preschool and school children in northeastern Thailand. Am. J. Epidemiol. 31:332-339. - PubMed
-
- Cantorna, M. T., F. E. Nashold, and C. E. Hayes. 1994. In vitamin A deficiency multiple mechanisms establish a regulatory T helper cell imbalance with excess Th1 and insufficient Th2 function. J. Immunol. 152:1515-1522. - PubMed
-
- Cantorna, M. T., F. E. Nashold, and C. E. Hayes. 1995. Vitamin A deficiency results in a priming environment conducive for Th1 cell development. Eur. J. Immunol. 25:1673-1679. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
