

Quantitation of immunoglobulin to hepatitis E virus by enzyme immunoassay
- PMID: 11986273
- PMCID: PMC120005
- DOI: 10.1128/cdli.9.3.639-648.2002
Quantitation of immunoglobulin to hepatitis E virus by enzyme immunoassay
Abstract
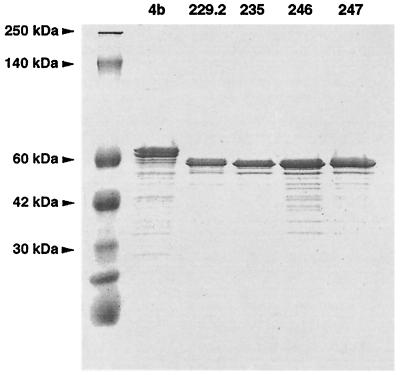
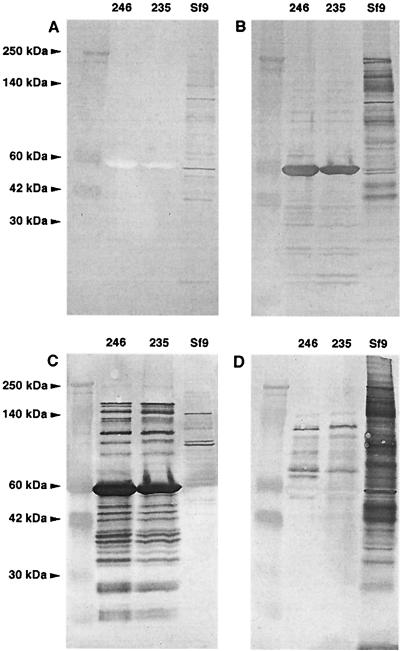
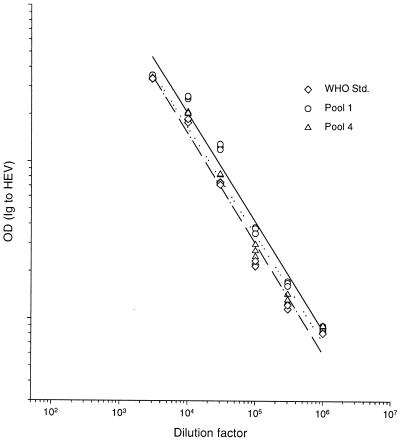
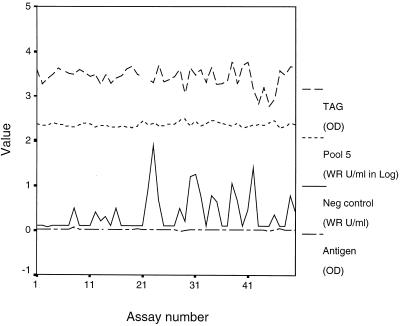
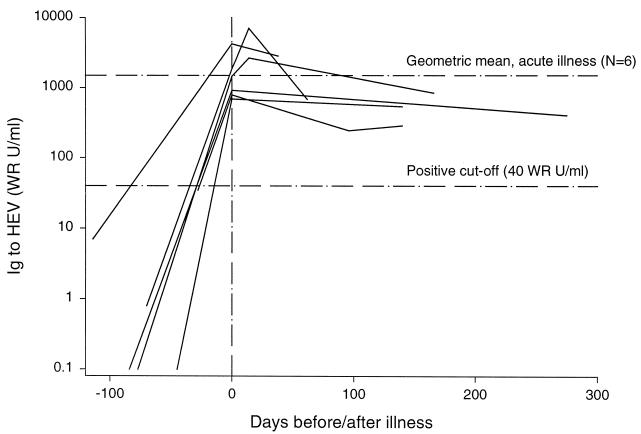
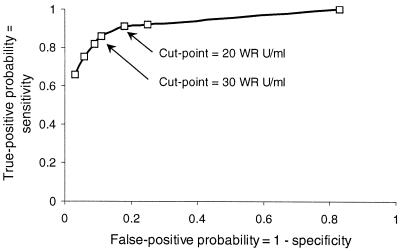
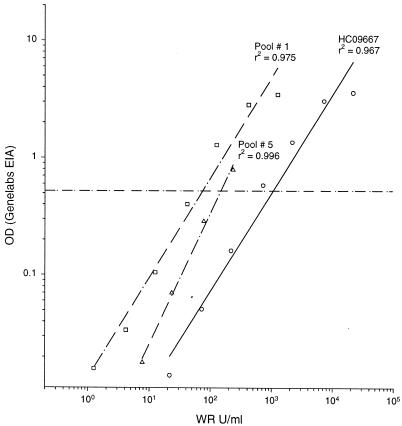
We developed a quantitative enzyme immunoassay (EIA) for antibody to hepatitis E virus (HEV) by using truncated HEV capsid protein expressed in the baculovirus system to improve seroepidemiology, to contribute to hepatitis E diagnosis, and to enable vaccine evaluations. Five antigen lots were characterized; we used a reference antiserum to standardize antigen potency. We defined Walter Reed antibody units (WR U) with a reference antiserum by using the four-parameter logistic model, established other reference pools as assay standards, and determined the conversion factor: 1 WR U/ml = 0.125 World Health Organization unit (WHO U) per ml. The EIA performed consistently; median intra- and inter-test coefficients of variation were 9 and 12%, respectively. The accurate minimum detection limit with serum diluted 1:1,000 was 5.6 WR U/ml; the test could detect reliably a fourfold antibody change. In six people followed from health to onset of hepatitis E, the geometric mean antibody level rose from 7.1 WR U/ml to 1,924.6 WR U/ml. We used the presence of 56- and 180-kDa bands by Western blotting as a confirmatory test and to define true-negative and -positive serum specimens. A receiver-operating characteristics plot identified 30 WR U/ml as an optimum cut-point (sensitivity, 86%; specificity, 89%). The EIA detected antibody more sensitively than a commercially available test. The EIA was transferred to another laboratory, where four operators matched reference laboratory results for a panel of unknowns. Quantitation of antibody to HEV and confirmation of its specificity by Western blotting make HEV serology more meaningful.
Figures

References
-
- Armitage, P., and G. Berry. 1987. Statistical methods in medical research, 2nd ed. Blackwell Scientific Publications, Boston, Mass.
-
- Bryan, J. P., S. A. Tsarev, M. Iqbal, J. Ticehurst, S. U. Emerson, A. Ahmed, J. Duncan, A. R. Rafiqui, I. A. Malik, R. H. Purcell, and L. J. Legters. 1994. Epidemic hepatitis E in Pakistan: patterns of serologic response and evidence that antibody to hepatitis E virus protects against disease. J. Infect. Dis. 170:517-521. - PubMed
-
- Clayson, E. T., K. S. Myint, R. Snitbhan, D. W. Vaughn, B. L. Innis, L. Chan, P. Cheung, and M. P. Shrestha. 1995. Viremia, fecal shedding, and IgM and IgG responses in patients with hepatitis E. J. Infect. Dis. 172:927-933. - PubMed
-
- Dawson, G. J., K. H. Chau, C. M. Cabal, P. O. Yarbough, G. R. Reyes, and I. K. Mushahwar. 1992. Solid-phase enzyme-linked immunosorbent assay for hepatitis E virus IgG and IgM antibodies utilizing recombinant antigens and synthetic peptides. J. Virol. Methods 38:175-186. - PubMed
-
- Favorov, M. O., H. A. Fields, M. A. Purdy, T. L. Yashina, A. G. Aleksandrov, M. J. Alter, D. M. Yarasheva, D. W. Bradley, and H. S. Margolis. 1992. Serologic identification of hepatitis E virus infection in epidemic and endemic settings. J. Med. Virol. 36:246-250. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
