

The Hospital for Sick Children, Toronto, Longitudinal ERG study of children on vigabatrin
- PMID: 11999622
- PMCID: PMC3880358
- DOI: 10.1023/a:1014656626174
The Hospital for Sick Children, Toronto, Longitudinal ERG study of children on vigabatrin
Abstract
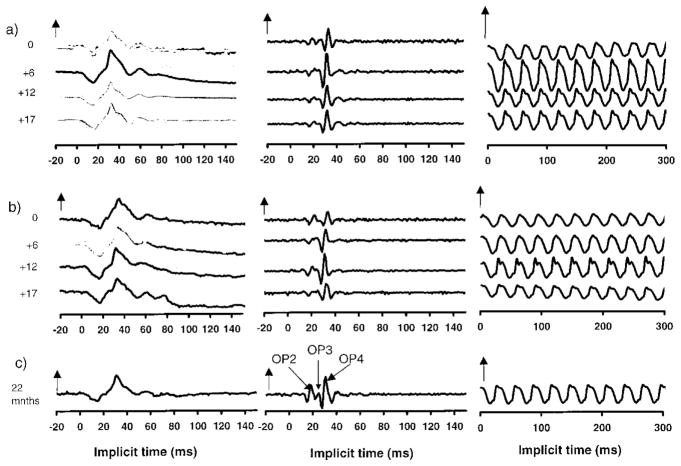
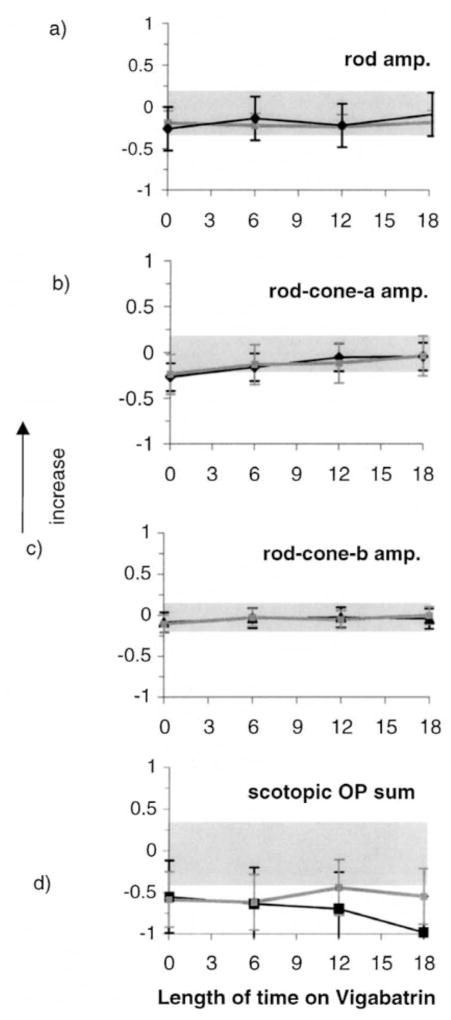
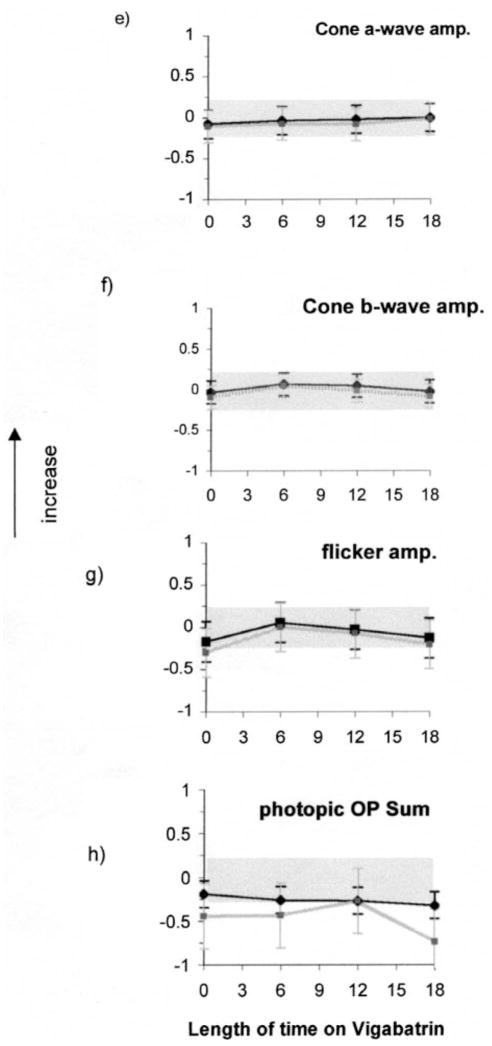
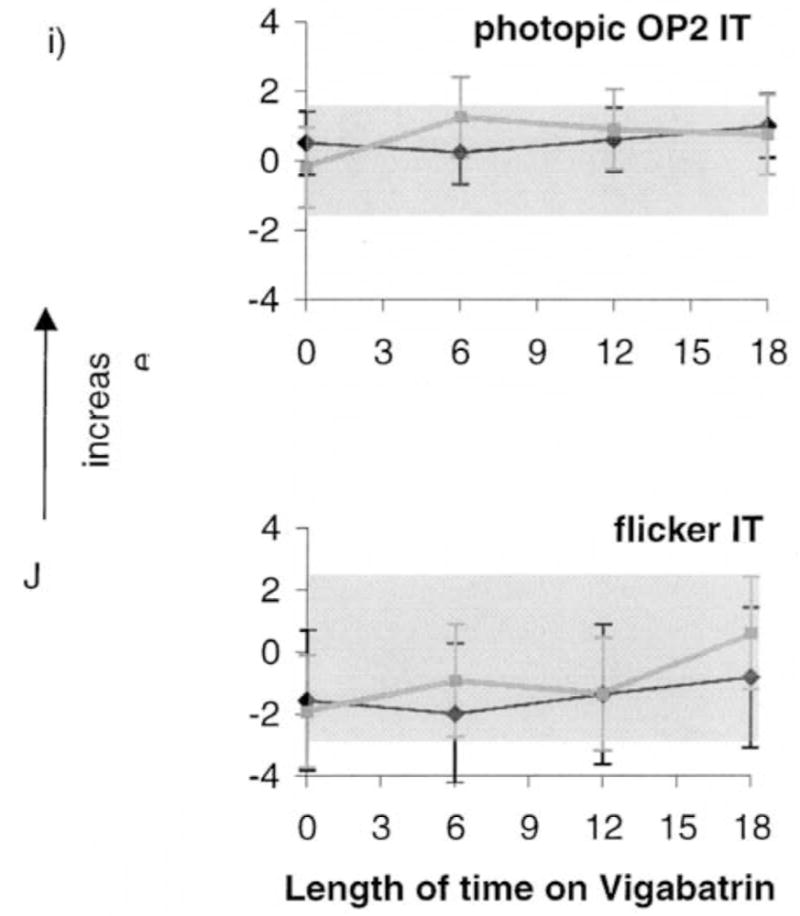
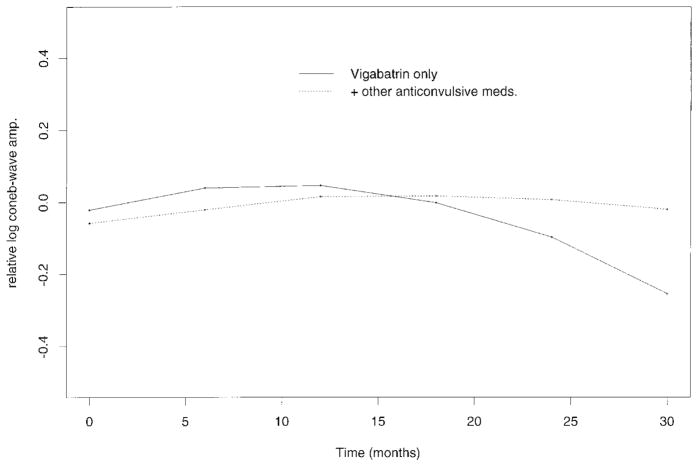
The purpose of this longitudinal study was to identify changes in ERG responses associated with vigabatrin treatment. We accomplished this by recording longitudinally ERGs in children before and during vigabatrin treatment and comparing results between children on vigabatrin monotherapy and those taking additional anticonvulsive medications. Thirty-three children on vigabatrin therapy were tested; the duration between visits was approximately 6 months. Thirteen children were assessed initially before starting vigabatrin therapy and seven were assessed soon after (age range 1.5-126 months, median 6 months). The remaining 13 patients were already on vigabatrin at the time of initial visit (age range 6.5-180 months, median 16 months). ERGs were tested using the standard protocol established by the International Society for Clinical Electrophysiology of Vision, with Burian-Allen bipolar contact-lens electrodes. In addition to standard responses we recorded photopic oscillatory potentials (OPs). All 33 patients were tested longitudinally on at least two occasions and 11 were tested on three occasions. For children whose only anticonvulsive drug was vigabatrin there was a significant curvature (quadratic function, p < 0.05) of the predicted cone b-wave amplitude with time; exhibited as increase in b-wave amplitude followed by subsequent decrease. Descriptive data demonstrated the same pattern in the group taking anticonvulsive medications in addition to vigabatrin. In most children the flicker amplitude declined between 6 months and 1 year of vigabatrin treatment. Our data demonstrated that rod responses, which may be abnormal before initiation of vigabatrin, did not change substantially with vigabatrin treatment.
Figures
References
-
- Fois A, Buoni S, Bartolo R, Marco V, Mostardini R. Vigabatrin treatment in children. Child’s Nerv Syst. 1994;10:244–48. - PubMed
-
- Kwong L. Vigabatrin as first line therapy in infantile spasms: review of seven patients. J Paediatr Child Health. 1997;33(2):121–4. - PubMed
-
- Uldall P, Alving J, Gram L, Beck S. Vigabatrin in pediatric epilepsy – an open study. J Child Neurol. 1991;6:2, S38–2S44. - PubMed
-
- Uldall P, Alving J, Gram L, Hogenhaven H. Vigabatrin in childhood epilepsy: a 5-year follow-up study. Neuropediatrics. 1995;26:253–56. - PubMed