

The appropriate use of carotid endarterectomy
- PMID: 12000252
- PMCID: PMC102359
The appropriate use of carotid endarterectomy
Abstract
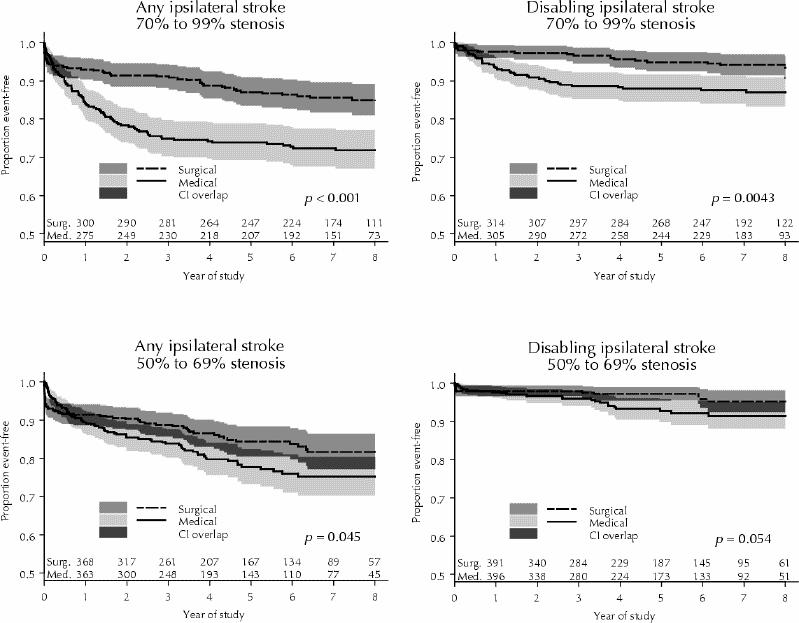
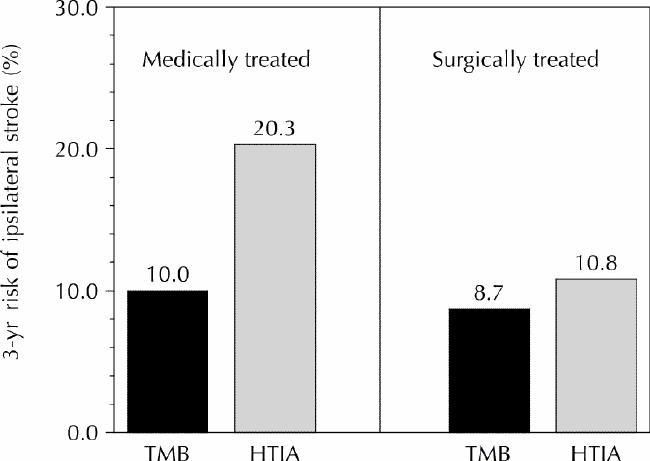
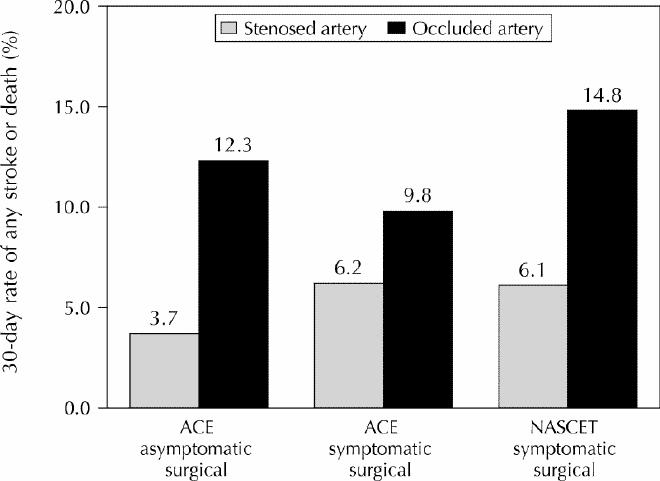
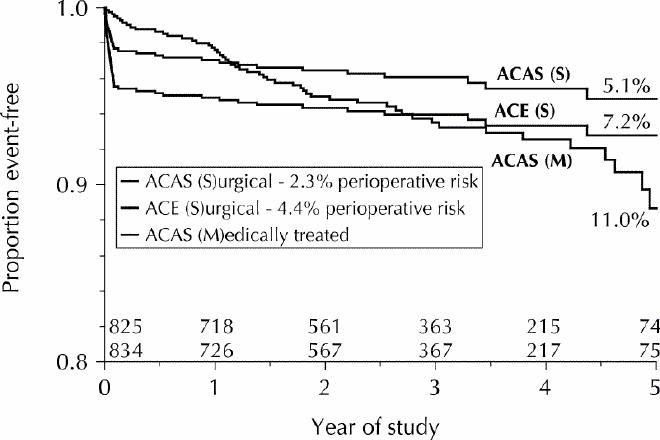
For the first 30 years after carotid endarterectomy was first developed, anecdotal evidence was used to identify patients with internal carotid artery disease for whom this procedure would be appropriate. More recently, the appropriateness of carotid endarterectomy for symptomatic patients and asymptomatic subjects has emerged from 7 randomized trials. Risk of stroke and benefit from the procedure are greatest for symptomatic patients with at least 70% stenosis of the internal carotid artery. Within this group, carotid endarterectomy is most beneficial for the following patients: otherwise healthy elderly patients, those with hemispheric transient ischemic attack, those with tandem extracranial and intracranial lesions and those without evidence of collateral vessels. Risk of perioperative stroke and death is higher in the following groups, although they still benefit: patients with widespread leukoaraiosis, those with occlusion of the contralateral internal carotid artery and those with intraluminal thrombus. Patients with 50% to 69% stenosis experience lesser benefit, and some other groups may even be harmed by carotid endarterectomy, including women and patients with transient monocular blindness only. The procedure is indicated for patients presenting with lacunar stroke and for those with a nearly occluded internal carotid artery, but the benefit is muted. Patients with less than 50% stenosis do not benefit. In the largest randomized trial of asymptomatic subjects, the perioperative risk of stroke and death was very low (1.5%), but the results indicated that a prohibitively high number of subjects (83) must be treated to prevent one stroke in 2 years. The subsequent literature reported higher perioperative risks (2.8% to 5.6%). In asymptomatic individuals nearly half of the strokes that occur may be due to heart and small-vessel disease. These limitations counter any potential benefit. Another trial is in progress and may identify subgroups of asymptomatic subjects who would benefit. Meanwhile, most individuals without symptoms fare better with medical care.
Figures
References
-
- Fields WS, Maslenikov V, Meyer JS, Hass WK, Remington RD, MacDonald M. Joint study of extracranial occlusion. V. Progress report of prognosis following surgery or nonsurgical treatment for transient cerebral ischemic attacks and cervical carotid artery lesions. JAMA 1970;211:1993-2003. - PubMed
-
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade stenosis. N Engl J Med 1991;325:445-53. - PubMed
-
- Barnett HJM, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al, for the North American Symptomatic Carotid Endarterectomy Trial Collaborators. Benefit of carotid endarterectomy in symptomatic patients with moderate and severe stenosis. N Engl J Med 1998;339:1415-25. - PubMed
-
- European Carotid Surgery Trialists' Group. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet 1998;351:1379-87. - PubMed
-
- Mayberg MR, Wilson SE, Yatsu F, Weiss DG, Messina L, Hershey LA, for the Veterans Affairs Cooperative Studies Program 309 Trialists Group. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA 1991;266:3289-94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical