

Case Reports
Intraarterial suction thrombectomy in acute stroke
Affiliations
- PMID: 12006277
- PMCID: PMC7974726
Item in Clipboard
Case Reports
Intraarterial suction thrombectomy in acute stroke
AJNR Am J Neuroradiol.
2002 May.
Abstract
Three patients with internal carotid artery thrombus and thrombolysis in myocardial infarction (TIMI) 0-1 flow were treated by using intraarterial (IA) suction thrombectomy a mean of 4.2 hours after stroke onset. After catheterization with a 7F guide-catheter, thrombus was aspirated by using a 60-mL syringe. TIMI flow improved to 3 in all patients. The median National Institutes of Health Stroke Scale score decreased from 22 (range, 12-23) to 4 (range, 2-22) at 3 months. IA suction thrombectomy may be safe and feasible in patients with acute stroke.
Figures
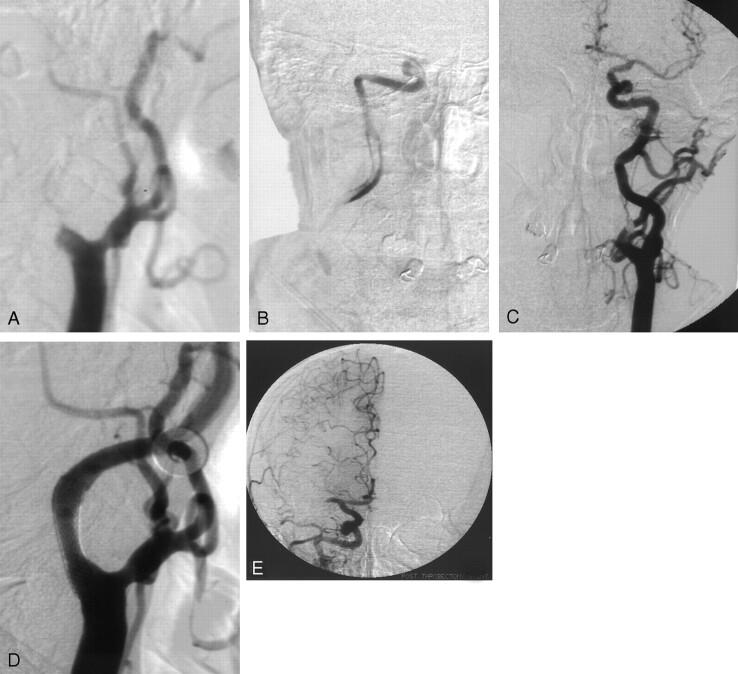
Case 1. A 67-year-old man presented with resolving left hemiparesis. A, Baseline right lateral common carotid artery (CCA) angiogram shows near-occlusion of the right ICA with a string sign of slow flow into the proximal ICA. B, After predilation of the proximal ICA stenosis, this baseline right ICA angiogram reveals the presence of extensive thrombus. C, Baseline left CCA angiogram reveals some right ACA cross-filling but no right MCA filling. D, Postprocedural right lateral CCA angiogram shows less than 20% residual ICA stenosis. A Wallstent in the ICA is visible at the carotid bifurcation. E, Although the right MCA has a persistent mid-M1 occlusion, the postprocedural right CCA angiogram shows good distal filling of the MCA branches via pial collaterals from the ACA.

Case 2. A 72-year-old man had global aphasia and right hemiparesis. A, Baseline left lateral CCA angiogram shows complete occlusion of the cervical ICA. Flow through a 50% stenosis of the external carotid artery remains visible. B, Postprocedural left lateral CCA angiogram demonstrates essentially complete resolution of the ICA occlusion. The Wallstent placed in the left ICA is visible at the carotid bifurcation.
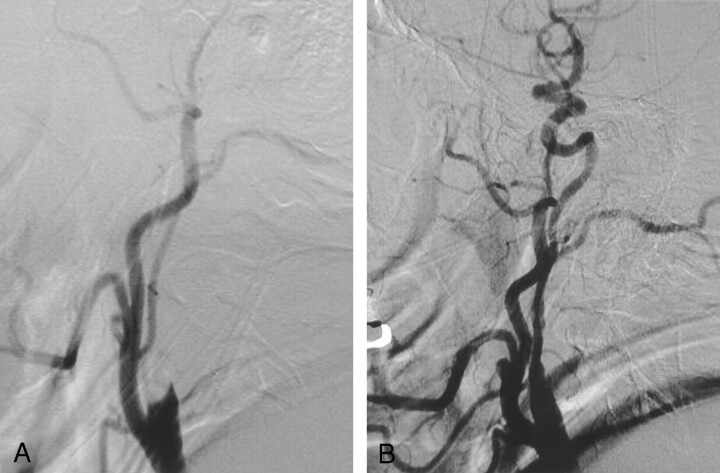
Case 3. A 49-year-old man with atrial fibrillation and a poor cardiac ejection fraction presented with left hemiparesis and right gaze preference A, Baseline right lateral CCA angiogram shows complete occlusion of the right ICA. B, Postprocedural right lateral CCA angiogram shows restored flow within the right ICA. A long segment of vessel narrowing is seen within the cervical ICA.
References
-
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581–1587 - PubMed
-
- Greenberg RK, Ouriel K, Srivastava S, et al. Mechanical versus chemical thrombolysis: an in vitro differentiation of thrombolytic mechanism. J Vasc Interv Radiol 2000;11:199–205 - PubMed
-
- Mori E, Yoneda Y, Tabuchi M, et al. Intravenous recombinant tissue plasminogen activator in acute carotid artery territory stroke. Neurology 1992;42:976–982 - PubMed
-
- Lutsep HL, Campbell M, Clark WM, et al. EPAR therapy system for treatment of acute stroke: safety study results. Stroke 2001;32:319b
-
- Wikholm G. Mechanical intracranial embolectomy: a report of two cases. Intervent Neuroradiol 1998;4:159–164 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical