

Central neural contribution to the perception of chest pain in cardiac syndrome X
- PMID: 12010930
- PMCID: PMC1767119
- DOI: 10.1136/heart.87.6.513
Central neural contribution to the perception of chest pain in cardiac syndrome X
Abstract
Objective: To investigate the central neural contribution to chest pain perception in cardiac syndrome X (angina-like pain, ECG changes during stress, angiographically normal coronary arteriogram).
Subjects: Eight syndrome X patients and eight healthy volunteers.
Methods: Dobutamine stress using echocardiography to assess myocardial function, and positron emission tomography to measure changes in regional cerebral blood flow, as an index of neuronal activity.
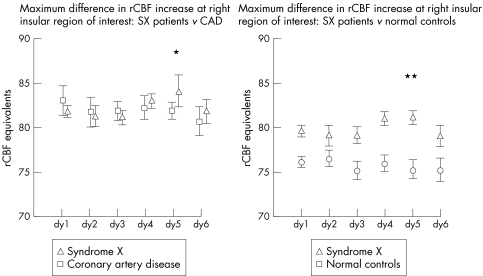
Results: During similar doses of dobutamine, syndrome X patients and controls showed comparable regional cerebral blood flow changes in the hypothalamus, thalami, right orbito-frontal cortex, and anterior temporal poles, associated with the sensation of a fast or powerful heart beat. In patients, but not controls, the stress also generated severe chest pain associated with increased activity in the right anterior insula/frontal operculum junction. There were ischaemia-like ECG changes in the syndrome X patients, but no left ventricular dysfunction on echocardiography. Activation of the right insula during chest pain clearly distinguished the syndrome X patients from a group of patients with known coronary disease.
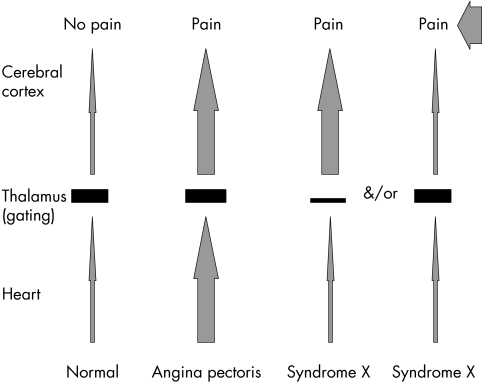
Conclusions: Chest pain and ECG changes were not accompanied by demonstrable myocardial dysfunction in syndrome X patients, but altered central neural handling of afferent signals may contribute to the abnormal pain perception in these patients.
Figures

Comment in
-
The complex link between brain and heart in cardiac syndrome X.Heart. 2002 Oct;88(4):328-30. doi: 10.1136/heart.88.4.328. Heart. 2002. PMID: 12231581 Free PMC article. No abstract available.
Similar articles
-
The brain-heart axis in the perception of cardiac pain: the elusive link between ischaemia and pain.Ann Med. 2000 Jul;32(5):350-64. doi: 10.3109/07853890008995938. Ann Med. 2000. PMID: 10949067 Clinical Trial.
-
Central nervous pathways mediating angina pectoris.Lancet. 1994 Jul 16;344(8916):147-50. doi: 10.1016/s0140-6736(94)92755-3. Lancet. 1994. PMID: 7912763
-
Silent ischemia as a central problem: regional brain activation compared in silent and painful myocardial ischemia.Ann Intern Med. 1996 Jun 1;124(11):939-49. doi: 10.7326/0003-4819-124-11-199606010-00001. Ann Intern Med. 1996. PMID: 8624061
-
Cardiac syndrome X. Diagnosis, pathogenesis and management.Am J Cardiovasc Drugs. 2004;4(3):179-94. doi: 10.2165/00129784-200404030-00005. Am J Cardiovasc Drugs. 2004. PMID: 15134470 Review.
-
[Microvascular angina and syndrome X].Rev Esp Cardiol. 2002;55 Suppl 1:10-6. Rev Esp Cardiol. 2002. PMID: 15626351 Review. Spanish.
Cited by
-
Gender and microvascular angina.J Thromb Thrombolysis. 2011 Jan;31(1):37-46. doi: 10.1007/s11239-010-0477-1. J Thromb Thrombolysis. 2011. PMID: 20419338 Free PMC article. Review.
-
Non-pharmacological Treatment of Refractory Angina and Microvascular Angina.Biomedicines. 2020 Aug 13;8(8):285. doi: 10.3390/biomedicines8080285. Biomedicines. 2020. PMID: 32823683 Free PMC article. Review.
-
Microvascular coronary dysfunction in women: pathophysiology, diagnosis, and management.Curr Probl Cardiol. 2011 Aug;36(8):291-318. doi: 10.1016/j.cpcardiol.2011.05.002. Curr Probl Cardiol. 2011. PMID: 21723447 Free PMC article. Review.
-
Women and Chest Pain: Recognizing the Different Faces of Angina in the Emergency Department.Yale J Biol Med. 2016 Jun 27;89(2):227-38. eCollection 2016 Jun. Yale J Biol Med. 2016. PMID: 27354848 Free PMC article. Review.
-
Cardiac syndrome X in women: the role of oestrogen deficiency.Heart. 2006 May;92 Suppl 3(Suppl 3):iii5-9. doi: 10.1136/hrt.2005.070318. Heart. 2006. PMID: 16614266 Free PMC article. Review.
References
-
- Cechetto DF. Supraspinal mechanisms of visceral representation. In: Gebhart GF, ed. Visceral pain, progress in pain research and management, vol 5. Seattle: IASP Press, 1995:261–90.
-
- Friston KJ, Frackowiak RSJ. Imaging functional anatomy. In: Lassen NA, Ingvar DH, Raichle ME, Friberg L, eds. Brain work and mental activity. Alfred Benzon symposium, vol 31. Copenhagen: Munksgaard, 1991:267–79.
-
- Rosen SD, Paulesu E, Frith CD, et al. Central neural correlates of angina pectoris as a model of visceral pain. Lancet 1994;344:147–50. - PubMed
-
- Rosen SD, Paulesu E, Nihoyannopoulos P, et al. Silent ischaemia as a central problem: regional brain activation compared in silent and painful myocardial ischaemia. Ann Intern Med 1996;124:939–49. - PubMed
-
- Epstein SE, Cannon RO. Site of increased resistance to coronary flow in patients with angina pectoris and normal epicardial coronary arteries. J Am Coll Cardiol 1986;8:459–61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical