

Review
doi: 10.1136/heart.87.6.575.
Novel mapping techniques for cardiac electrophysiology
Affiliations
- PMID: 12010949
- PMCID: PMC1767151
- DOI: 10.1136/heart.87.6.575
Item in Clipboard
Review
Novel mapping techniques for cardiac electrophysiology
Heart.
2002 Jun.
No abstract available
Figures
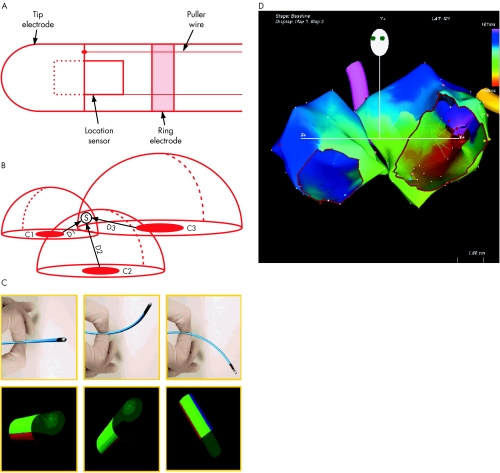
Electroanatomic mapping. (A) The catheter is composed of tip and ring electrodes and a location sensor embedded within the catheter. (B) A location pad with three coils (C1, C2, and C3) generates magnetic fields that decay as a function of distance from the coils. The sensor measures the strength of each field, permitting determination of the distance from each coil (D1, D2, D3). The intersection of three theoretical spheres of radii D1, D2, and D3 determines the catheter tip location in space. Reproduced from Gepstein et al, with permission. (C) Deflection of the catheter in space (top panels) results in real time display of catheter orientation on the computer screen, to guide non-fluoroscopic manipulation. (D) Activation map from a patient with left atrial figure of eight re-entrant tachycardia. The two atria are shown in the left anterior oblique view, with tricuspid valve and mitral valve cut out. The colour at each anatomic point shows local activation time relative to the reference catheter (scale top right).
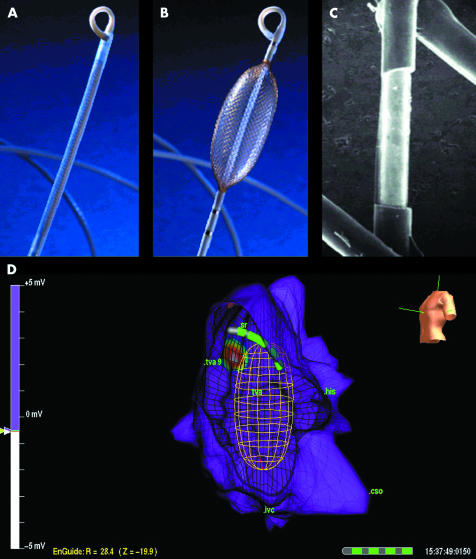
Non-contact system multiple electrode array (MEA). (A) In low profile, the MEA is advance through the vasculature to the chamber of interest. (B) After deployment in the chamber of interest, the MEA is expanded to record intracavitary potentials. (C) Photomicrograph of the MEA showing one of the 64 laser etched laser etched unipolar electrodes. (D) Right atrial map in a patient with ectopic tachycardia. Left anterior oblique view is shown. Point of earliest activation is shown (white centre of target). On computer workstation, activation “movie” depicts wavefront propagation. The position of mapping catheter relative to the atrial geometry is shown by means of the locator signal.
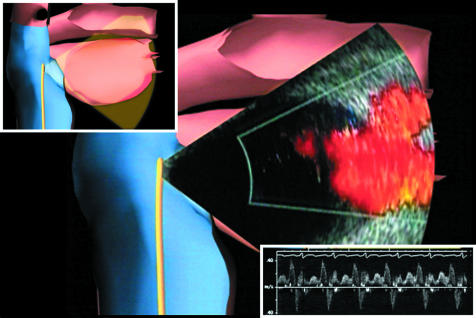
Phased array intracardiac echocardiography to image the left sided pulmonary veins with colour flow Doppler. Actual echocardiographic image is superimposed on computer model for orientation. Inset top left: computer graphic to depict ICE catheter position within the right atrium. Inset bottom right: pulse wave Doppler to quantify left superior pulmonary vein flow. This appears to be a sensitive indicator of venous stenosis during ablation. Reproduced from Darbar et al, with permission.
References
-
- Darbar D, Olgin J, Miller J, et al. Localization of the origin of arrhythmias for ablation: from electrocardiography to advanced endocardial mapping systems. J Cardiovasc Electrophysiol 2001;12:1309–25. ▸ Recent review of advanced mapping systems and intracardiac imaging. - PubMed
-
- Schalij MJ, van Rugge FP, Siezenga M, et al. Endocardial activation mapping of ventricular tachycardia in patients : first application of a 32-site bipolar mapping electrode catheter. Circulation 1998;98:2168–79. - PubMed
-
- Kottkamp H, Hindricks G, Breithardt G, et al. Three-dimensional electromagnetic catheter technology: electroanatomical mapping of the right atrium and ablation of ectopic atrial tachycardia. J Cardiovasc Electrophysiol 1997;8:1332–7. - PubMed
-
- Nakagawa H, Shah N, Matsudaira K, et al. Characterization of reentrant circuit in macroreentrant right atrial tachycardia after surgical repair of congenital heart disease: isolated channels between scars allow “focal” ablation. Circulation 2001;103:699–709. ▸ Elegant paper describing the presence of multiple narrow channels as vulnerable ablation targets in patients with congenital heart disease and previous surgery, and use of electroanatomic mapping to localise them. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources