

Resource utilization related to atrial fibrillation after coronary artery bypass grafting
- PMID: 12022486
- PMCID: PMC3674411
Resource utilization related to atrial fibrillation after coronary artery bypass grafting
Abstract
Background: Studies of resource utilization by patients with new-onset atrialfibrillation after coronary artery bypass grafting have addressed only length of stay and bed charges.
Objective: To compare resource utilization between patients with new-onset atrial fibrillation and patients without atrialfibrillation after isolated coronary artery bypass grafting.
Methods: Retrospective review of clinical and administrative electronic databases for 720 subjects who underwent isolated coronary artery bypass grafting with cardiopulmonary bypass in 25 months at one medical center The prevalence of atrial fibrillation was determined, and resource utilization in various hospital cost centers was compared between subjects with and without atrialfibrillation.
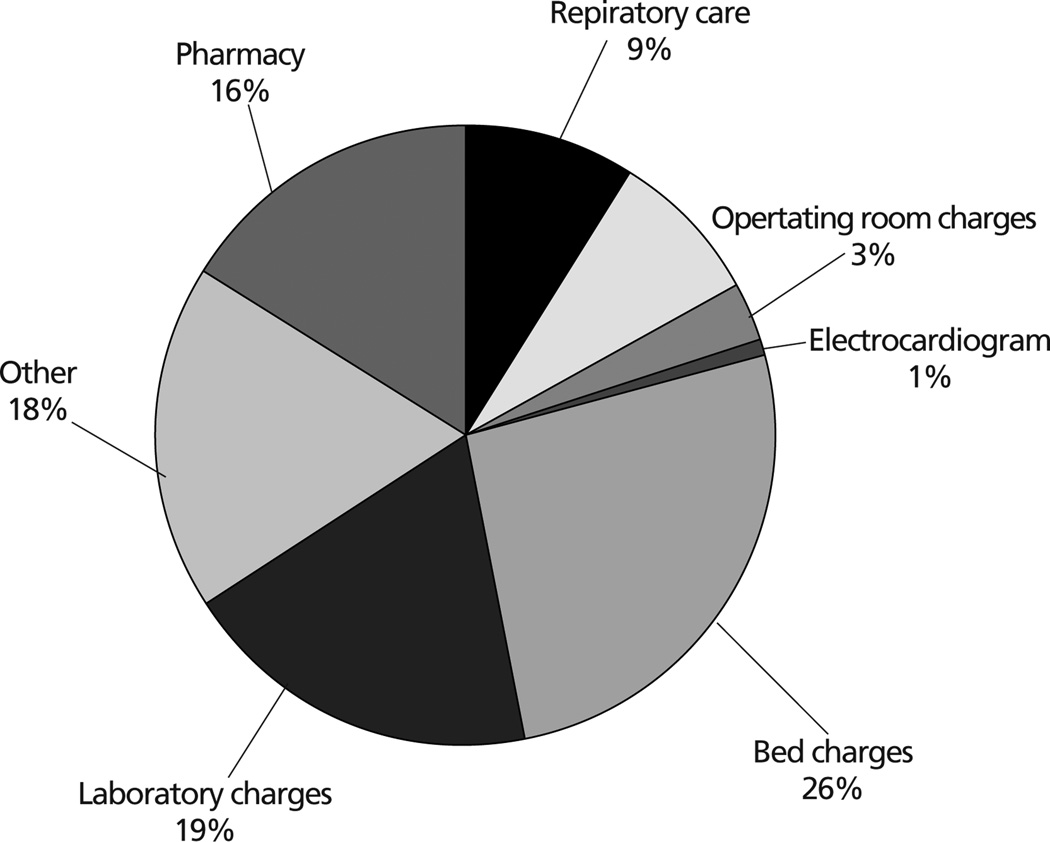
Results: The prevalence of new-onset atrial fibrillation was 33.1%. Compared with subjects without atrialfibrillation, subjects with atrialfibrillation had a longer stay (5.8 +/- 2.4 vs. 4.4+/-1.2 days, P<.001), more days receiving mechanical ventilation (P =.002) and oxygen therapy (P<.001), and higher rates of readmission to the intensive care unit (4.6% vs. 0.2%, P<.001). Subjects with atrial fibrillation also had more laboratory tests (P<.001) and more days receiving cardiac drugs, heparin, diuretics, and electrolytes. Subjects with atrialfibrillation had higher total postoperative charges ($57261 +/- $17101 vs. $50905 +/- $10062, P = .001), a mean difference of $6356. The mean differences were greatest for bed charges ($1642), laboratory charges ($1215), pharmacy ($989), and respiratory care ($582).
Conclusion: The economic impact of atrialfibrillation after coronary artery bypass grafting has been underestimated.
Figures
Comment in
-
Resource utilization related to atrial fibrillation after coronary artery bypass grafting (May 2002:228-238).Am J Crit Care. 2002 Nov;11(6):501; author reply 501-2. Am J Crit Care. 2002. PMID: 12425399 No abstract available.
References
-
- Olshansky B. Management of atrial fibrillation after coronary artery bypass graft. Am J Cardiol. 1996;78:27–34. - PubMed
-
- Bietz DS. Rapid recovery in the elderly. Ann Thorac Surg. 1997;64:1222–1223. - PubMed
-
- Kowey PR, Dallessandro DA, Herbertson R, et al. Effectiveness of digitalis with or without acebutolol in preventing atrial arrhythmias after coronary artery surgery. Am J Cardiol. 1997;79:1114–1117. - PubMed
-
- Mathew JP, Parks R, Savino JS, et al. Atrial fibrillation following coronary artery bypass graft surgery: predictors, outcomes and resource utilization. JAMA. 1996;276:300–306. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical