

Main pancreatic ductal anatomy can direct choice of modality for treating pancreatic pseudocysts (surgery versus percutaneous drainage)
- PMID: 12035030
- PMCID: PMC1422503
- DOI: 10.1097/00000658-200206000-00001
Main pancreatic ductal anatomy can direct choice of modality for treating pancreatic pseudocysts (surgery versus percutaneous drainage)
Abstract
Objective: To test the hypothesis that pancreatic ductal anatomy may predict the likely success of percutaneous drainage of pseudocysts of the pancreas.
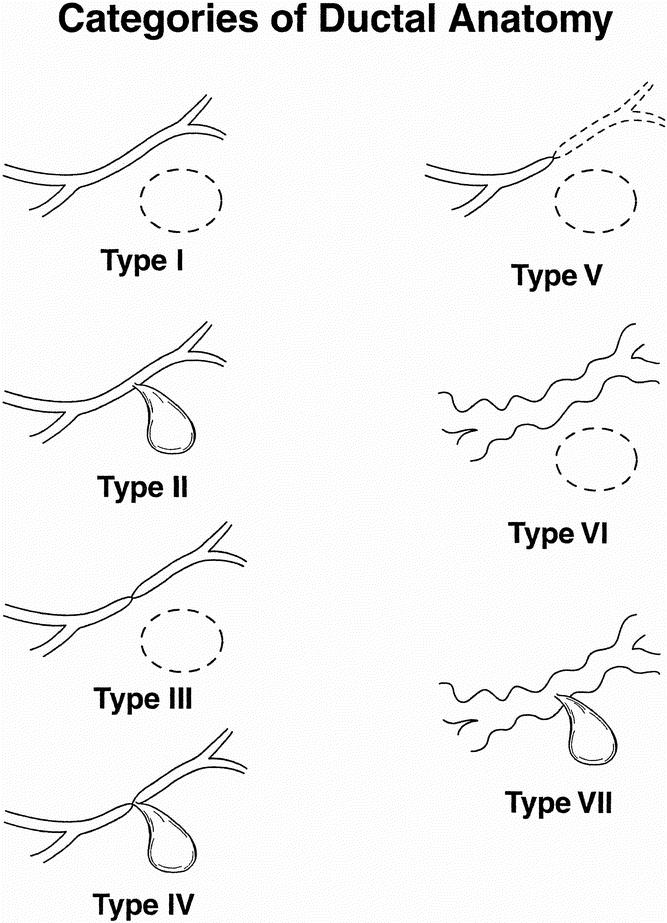
Summary background data: Various modalities are currently applied to pseudocysts, with little or no data to aid in the choice of management strategy. Pancreatic ductal anatomy was assessed and a system to categorize ductal changes was established.
Methods: Patients with a diagnosis of pancreatic pseudocyst were evaluated from 1985 to 2000. Two hundred fifty-three patients have been included in this series. Pancreatic ductal anatomy was defined using endoscopic retrograde cholangiopancreatography and categorized as a normal duct, a stricture, or complete cut-off of the pancreatic duct. Communication between the duct and cyst was noted.
Results: Among the 253 patients, 68 (27%) had spontaneous resolution. Fifty of the remaining 185 had percutaneous drainage and 148 (13 of whom failed to respond to percutaneous drainage) had surgery. There were no deaths in either group. Mean length of time with catheter drainage among all percutaneous drainage patients was 79.2 +/- 19.6 days. Patients with normal pancreatic ducts and those with strictures but no communication between the duct and the cyst who had percutaneous drainage had a much shorter length of hospital stay (6.1 +/- 4.6 days) than patients with strictures and duct-cyst communication and patients with complete cut-off of the duct (33.5 +/- 5.2 days and 39.1 +/- 7.9 days, respectively). Length of drainage also correlated with ductal anatomy. All patients with chronic pancreatitis failed to respond to percutaneous drainage.
Conclusions: Pancreatic ductal anatomy provides a clear correlation with the failure and successes of pseudocysts managed by percutaneous drainage as well as predicting the total length of drainage. Percutaneous drainage is best applied to patients with normal ducts and is acceptably applied to patients with stricture but no cyst-duct communication.
Figures
References
-
- Bradley E, Clements JL Jr, Gonzales AC. The natural history of pancreatic pseudocysts: a unified concept of management. Am J Surg 1979; 137: 135–141. - PubMed
-
- D’Egidio A, Schein, M. Pancreatic pseudocysts: a Proposed classification and its management implications. Br J Surg 1999; 78: 981–984. - PubMed
-
- Van Sonnenberg E, Wittich GR, Casola G, et al. Percutaneous drainage of infected and noninfected pancreatic pseudocysts: experience in 101 cases. Radiology 1989; 170: 757–761. - PubMed
-
- Criadoe Desterano AA, Weiner TM, Jacques PF. Long-term results of percutaneous catheter drainage of pancreatic pseudocysts. Surg Gynecol Obstet 1992; 175: 293–297. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
