

Mechanical methods of reducing blood transfusion in cardiac surgery: randomised controlled trial
- PMID: 12039820
- PMCID: PMC113763
- DOI: 10.1136/bmj.324.7349.1299
Mechanical methods of reducing blood transfusion in cardiac surgery: randomised controlled trial
Erratum in
- BMJ 2002 Jul 20;325(7356):142
Abstract
Objective: To assess the effectiveness of two mechanical methods of blood conservation in reducing the need for allogeneic red blood cells or coagulation products during cardiac surgery.
Design: Randomised controlled trial.
Setting: Regional cardiac centre in a teaching hospital in Southampton.
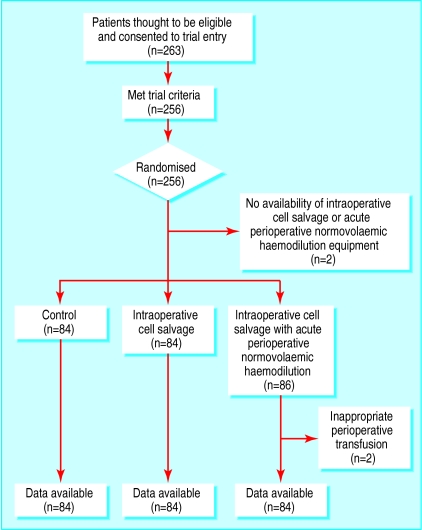
Participants: 263 adults aged 18-80 years undergoing elective coronary artery bypass surgery entered the study, of whom 252 completed the trial. All patients received routine perioperative care. Patients were allocated to one of three treatment groups: intraoperative cell salvage, intraoperative cell salvage with acute perioperative normovolaemic haemodilution, or no mechanical blood conservation. There were 84 patients in each group.
Main outcome measures: Numbers of patients who received allogeneic blood or coagulation products, and the mean number of units of blood transfused per patient.
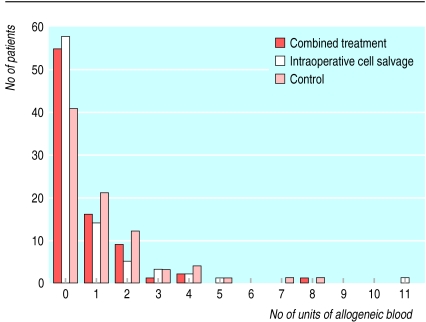
Results: Of the patients in the intraoperative cell salvage group, 26 were given a transfusion of allogeneic blood, compared with 43 in the control group (odds ratio 0.43 (95% confidence interval 0.23 to 0.80)). The mean number of units of allogeneic blood transfused per patient in the intraoperative cell salvage group was 0.68 units (SD=1.55), compared with 1.07 (1.56) units in the control group. 32 of the patients in the intraoperative cell salvage group were given any blood product, compared with 47 in the control group (odds ratio 0.47 (0.25 to 0.89); P=0.019). Combining acute perioperative normovolaemic haemodilution with intraoperative cell salvage conferred no additional benefits.
Conclusions: An intraoperative cell salvage device should be used in elective coronary artery bypass grafting. Pharmacological strategies may achieve further reductions in blood transfusions. Yet further reductions in blood transfusions could be achieved if the lower safe limit of haemoglobin concentration in patients undergoing cardiac surgery were known.
Figures
Comment in
-
Reducing blood transfusion. BMJ 's cover and headline exaggerated importance of study's findings.BMJ. 2002 Sep 21;325(7365):655. BMJ. 2002. PMID: 12242182 Free PMC article. No abstract available.
-
Reducing blood transfusion. Cell salvage reduces blood use, but does it do so on its own?BMJ. 2002 Sep 21;325(7365):655. BMJ. 2002. PMID: 12269317 No abstract available.
-
Reducing blood transfusion. Some important points were missing from the study.BMJ. 2002 Sep 21;325(7365):655. BMJ. 2002. PMID: 12269318 No abstract available.
-
Reducing blood transfusion. Focus should be on improving patients' ability to make own blood.BMJ. 2002 Sep 21;325(7365):655. BMJ. 2002. PMID: 12269319 No abstract available.
References
-
- National Blood Authority. Annual report 2000. www.blood.co.uk/pages/f24Pubs.html.
-
- Killip T. Twenty years of coronary bypasss surgery. N Engl J Med. 1988;319:366–368. - PubMed
-
- Renton MC, McClelland DB, Sinclair CJ. Use of blood products in cardiac surgery. Perfusion. 1997;3:157–162. - PubMed
-
- Dalrymple-Hay MJ, Pack L, Deakin CD, Shephard S, Ohri SK, Haw MP, et al. Autotransfusion of washed shed mediastinal fluid decreases the requirement for autologous blood transfusion following cardiac surgery: a prospective randomised trial. Eur J Cardiothorac Surg. 1999;15:830–834. - PubMed
-
- Schreiber G, Busch M, Kleinman S, Korelitz J. The risk of transfusion-transmitted viral infections. N Engl J Med. 1996;334:1685–1690. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical