

Cost effectiveness analysis of different approaches of screening for familial hypercholesterolaemia
- PMID: 12039822
- PMCID: PMC113765
- DOI: 10.1136/bmj.324.7349.1303
Cost effectiveness analysis of different approaches of screening for familial hypercholesterolaemia
Abstract
Objectives: To assess the cost effectiveness of strategies to screen for and treat familial hypercholesterolaemia.
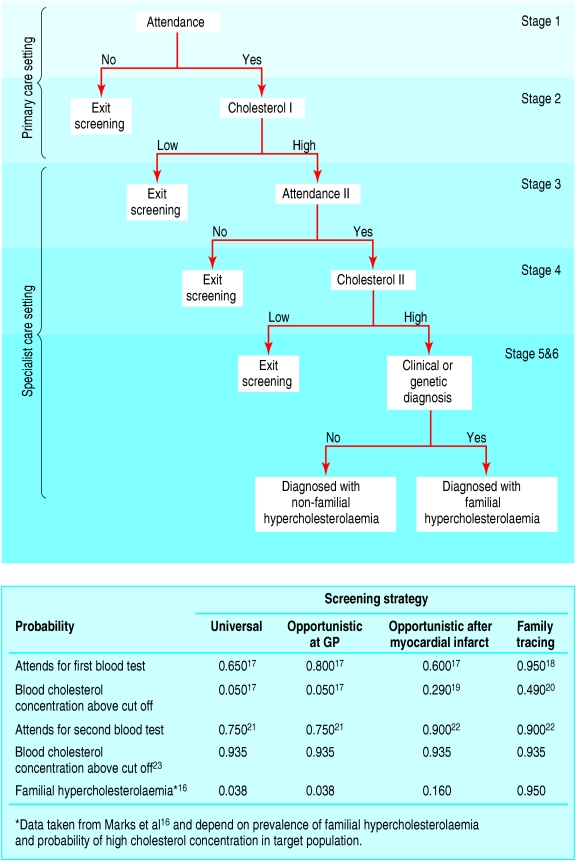
Design: Cost effectiveness analysis. A care pathway for each patient was delineated and the associated probabilities, benefits, and costs were calculated.
Participants: Simulated population aged 16-54 years in England and Wales.
Interventions: Identification and treatment of patients with familial hypercholesterolaemia by universal screening, opportunistic screening in primary care, screening of people admitted to hospital with premature myocardial infarction, or tracing family members of affected patients.
Main outcome measure: Cost effectiveness calculated as cost per life year gained (extension of life expectancy resulting from intervention) including estimated costs of screening and treatment.
Results: Tracing of family members was the most cost effective strategy (3097 pounds sterling (euros 5066, $4479) per life year gained) as 2.6 individuals need to be screened to identify one case at a cost of 133 pounds sterling per case detected. If the genetic mutation was known within the family then the cost per life year gained (4914 pounds sterling ) was only slightly increased by genetic confirmation of the diagnosis. Universal population screening was least cost effective (13 029 pounds sterling per life year gained) as 1365 individuals need to be screened at a cost of 9754 pounds sterling per case detected. For each strategy it was more cost effective to screen younger people and women. Targeted strategies were more expensive per person screened, but the cost per case detected was lower. Population screening of 16 year olds only was as cost effective as family tracing (2777 pounds sterling with a clinical confirmation).
Conclusions: Screening family members of people with familial hypercholesterolaemia is the most cost effective option for detecting cases across the whole population.
Comment in
-
Another way of screening for familial hypercholesterolaemia.BMJ. 2002 Aug 10;325(7359):340. doi: 10.1136/bmj.325.7359.340. BMJ. 2002. PMID: 12169521 Free PMC article. No abstract available.
References
-
- Goldstein JL, Brown MS. Familial hypercholesterolaemia. In: Scriver CR, Beudet AL, Sly WS, Valle D, editors. The metabolic basis of inherited disease. New York: McGraw Hill; 1995. pp. 1215–1245.
-
- Slack J. Risks of ischaemic heart-disease in familial hyperlipoproteinaemic states. Lancet. 1969;2:1380–1382. - PubMed
-
- Stone NJ, Levy RI, Fredrickson DS, Verter J. Coronary artery disease in 116 kindred with familial type II hyperlipoproteinemia. Circulation. 1974;49:476–488. - PubMed
-
- Scientific Steering Committee on behalf of the Simon Broome Register Group. Mortality in treated heterozygous familial hypercholesterolaemia: implications for clinical management. Atherosclerosis. 1999;142:105–112. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources