

Effect of a scoring system and protocol for sedation on duration of patients' need for ventilator support in a surgical intensive care unit
- PMID: 12052813
- PMCID: PMC1123333
- DOI: 10.1136/bmj.324.7350.1386
Effect of a scoring system and protocol for sedation on duration of patients' need for ventilator support in a surgical intensive care unit
Abstract
Problem: Need for improved sedation strategy for adults receiving ventilator support.
Design: Observational study of effect of introduction of guidelines to improve the doctors' and nurses' performance. The project was a prospective improvement and was part of a national quality improvement collaborative.
Background and setting: A general mixed surgical intensive care unit in a university hospital; all doctors and nurses in the unit; all adult patients (>18 years) treated by intermittent positive pressure ventilation for more than 24 hours.
Key measures for improvement: Reduction in patients' mean time on a ventilator and length of stay in intensive care over a period of 11 months; anonymous reporting of critical incidents; staff perceptions of ease and of consequences of changes.
Strategies for change: Multiple measures (protocol development, educational presentations, written guidelines, posters, flyers, emails, personal discussions, and continuous feedback) were tested, rapidly assessed, and adopted if beneficial.
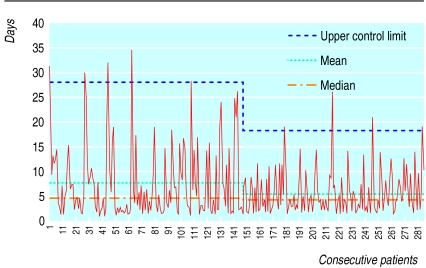
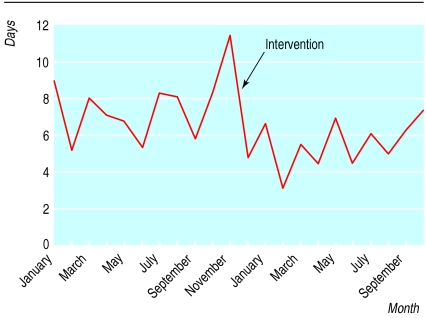
Effects of change: Mean ventilator time decreased by 2.1 days (95% confidence interval 0.7 to 3.6 days) from 7.4 days before intervention to 5.3 days after. Mean stay decreased by 1.0 day (-0.9 to 2.9 days) from 9.3 days to 8.3 days. No accidental extubations or other incidents were identified.
Lessons learnt: Relatively simple changes in sedation practice had significant effects on length of ventilator support. The change process was well received by the staff and increased their interest in identifying other areas for improvement.
Figures
References
-
- Kollef MH, Levy NT, Ahrens TS, Schaiff R, Prentice D, Sherman G. The use of continuous i.v. sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114:541–548. - PubMed
-
- Kollef MH, Horst HM, Prang L, Brock WA. Reducing the duration of mechanical ventilation: three examples of change in the intensive care unit. New Horiz. 1998;6:52–60. - PubMed
-
- Marx WH, DeMaintenon NL, Mooney KF, Mascia ML, Medicis J, Franklin PD, et al. Cost reduction and outcome improvement in the intensive care unit. J Trauma. 1999;46:625–630. - PubMed
-
- Plsek PE. Quality improvement methods in clinical medicine. Pediatrics. 1999;103:203–214. - PubMed
-
- Rainey TG, Kabcenell A, Berwick DM, Roessner J. Breakthrough series guide: reducing costs and improving outcomes in adult intensive care. Boston: Institute for Healthcare Improvement; 1998.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials