

Case Reports
Indolent intracranial mucormycosis: case report
Affiliations
- PMID: 12063219
- PMCID: PMC7976923
Item in Clipboard
Case Reports
Indolent intracranial mucormycosis: case report
AJNR Am J Neuroradiol.
2002 Jun-Jul.
Abstract
We present a patient with isolated intracranial mucormycosis that remained indolent for several months. The mucormycosis formed a mass in the prepontine cistern, probably spreading from the sphenoid sinus. We propose that at least some cases of what is considered isolated CNS mucormycosis develop from such unrecognized indolent infections. Mucormycosis may present as a mass in the basilar cisterns, especially in immunocompromised patients.
Figures
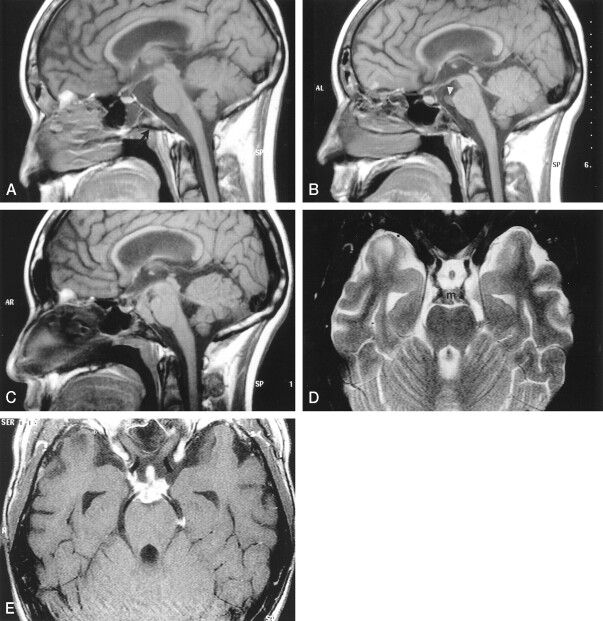
Images from the case of a 16-year-old male patient with acute lymphatic leukemia who was treated with unrelated bone marrow transplant and developed graft versus host disease. A, Midsagittal spin-echo T1-weighted image (550/12 [TR/TE]; matrix, 256 × 218; field of view, 230; section thickness, 5 mm) shows subtle areas of decreased signal intensity in the bone marrow (arrow) of the clivus. For a 16-year-old patient, the signal may still be heterogenous; however, this is more prominent than is usually seen. The prepontine cistern is normal. The sphenoid sinus contains a fluid level. The lateral ventricles are prominent. B, Corresponding T1-weighted image obtained 3 months after the image shown in A shows further decrease in signal intensity involving most of the clivus. There is mucosal thickening in the adjacent posterior aspect of the sphenoid sinus. A tract extending horizontally from this thickened mucosa through the clivus appears to be present. A small soft-tissue mass (arrowhead) in the superior aspect of the prepontine cistern adjacent to the basilar artery is seen. C, Image obtained 9 months after the image shown in B shows that the mass has grown and fills most of the prepontine and interpeduncular cisterns. The pituitary stalk is also thick. The bone marrow throughout the clivus is markedly hypointense, and there is mucosal thickening and an irregular rim in the posterior aspect of the sphenoid sinus. The ventricular size is unchanged. D, Axial view fast spin-echo T2-weighted image (5500/96; field of view, 200; matrix, 512 × 256; section thickness, 3 mm), obtained at the same time as the image shown in C, shows that the mass (m) is of low signal intensity and extends along the posterior cerebral arteries and posterior communicating arteries. The thick pituitary stalk is seen within the suprasellar cistern. E, Axial view contrast-enhanced spin-echo T1-weighted image (850/14; field of view, 200; matrix, 512 × 256; section thickness, 3 mm) shows intense enhancement of the mass and its extension to the pituitary stalk. The enhancing mass spreads along the internal carotid artery on the right and into the left ambient cistern.
References
-
- Gamba JL, Woodruff WW, Djang WT, Yeates et al. Craniofacial mucormycosis: assessment with CT. Radiology 1986;160:207–212 - PubMed
-
- Fatterpekar G, Mukherji S, Arbealez A, Maheshwari S, Castillo M. Fungal diseases of the paranasal sinuses. Semin Ultrasound CT MR 1999;20:391–401 - PubMed
-
- Terk MR, Underwood DJ, Zee C, Colletti PM. MR imaging in rhinocerebral and intracranial mucormycosis with CT and pathologic correlation. Magn Reson Imaging 1992;10:81–87 - PubMed
-
- Harril WC, Stewart MG, Lee AG, Cernoch P. Chronic rhinocerebral mucormycosis. Laryngoscope 1996;106:1292–1297 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical