

Pharmacology of acid suppression in the hospital setting: focus on proton pump inhibition
- PMID: 12072661
- PMCID: PMC6736586
- DOI: 10.1097/00003246-200206001-00003
Pharmacology of acid suppression in the hospital setting: focus on proton pump inhibition
Abstract
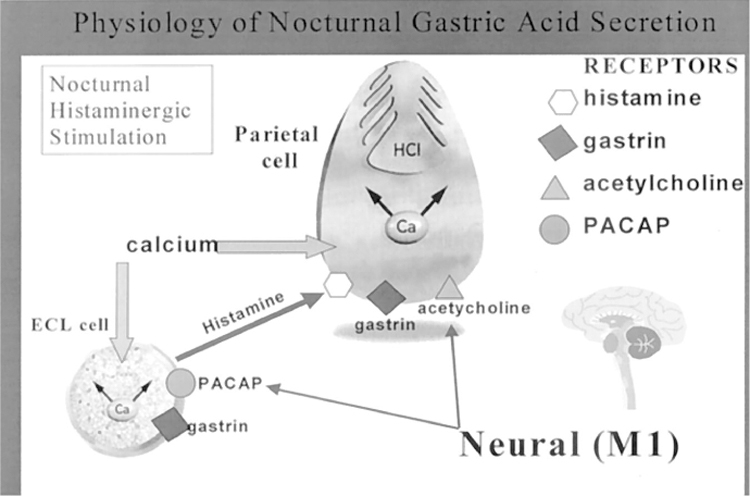
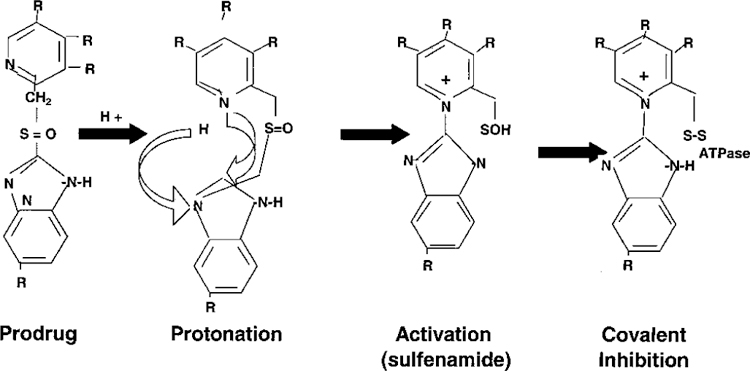
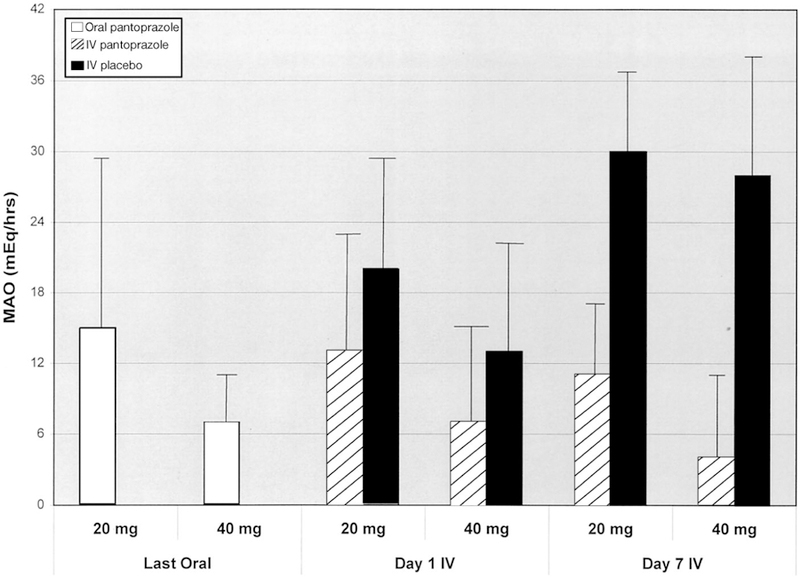
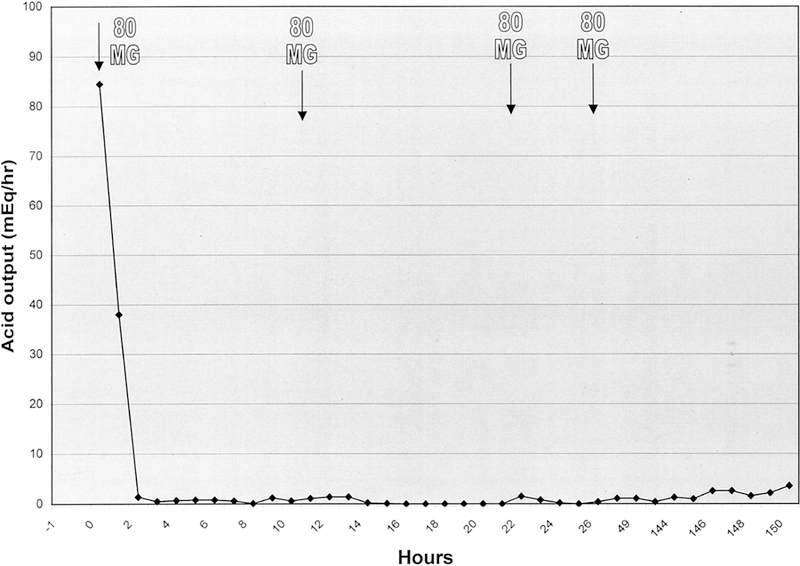
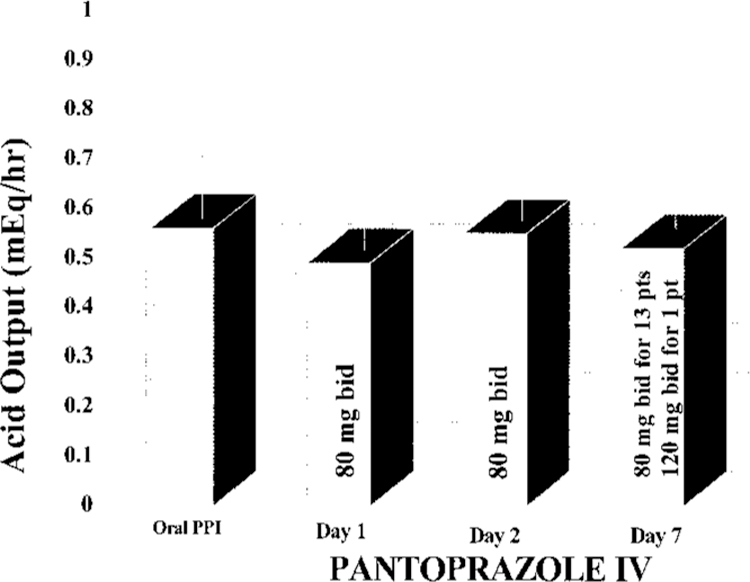
The more potent and longer-lasting inhibition of gastric acid secretion provided by proton pump inhibitors (PPIs) as compared with histamine-2-receptor antagonists is caused in large part by differences in their mechanism of action. PPIs block histamine-2-, gastrin-, and cholinergic-mediated sources of acid production and inhibit gastric secretion at the final common pathway of the H+/K+ adenosine triphosphatase proton pump. In contrast, histamine-2-receptor antagonists cannot block receptor sites other than those mediated by histamine. It seems that the rapid loss of acid suppression activity by the histamine-2-receptor antagonists may be attributed to tolerance. Such tolerance has not occurred in patients receiving PPIs because these agents are irreversible inhibitors of the H+/K+ adenosine triphosphatase proton pump. For these reasons, patients who have acid-related disorders that require high levels of acid suppression do not respond well to intravenous histamine-2-receptor antagonists and would be excellent candidates for intravenous PPI therapy. Candidates for intravenous PPIs also include patients who cannot receive oral PPIs and those who may need the higher acid suppression therapy provided by the intravenous rather than the oral route. Clinical studies have demonstrated the efficacy of intravenous pantoprazole in maintaining adequate control of gastric acid output during the switch from oral to intravenous therapy in patients with severe gastroesophageal reflux disease or the Zollinger-Ellison syndrome. Intragastric administration of solutions prepared from oral PPIs has been used as an alternative to the intravenous route in critical care settings. However, decreased bioavailability may limit the value of intragastric delivery of PPIs because of the high frequency of gastric emptying problems in critically ill patients.
Figures
Similar articles
-
Evaluation of omeprazole, lansoprazole, pantoprazole, and rabeprazole in the treatment of acid-related diseases.J Am Pharm Assoc (Wash). 2000 Jan-Feb;40(1):52-62; quiz 121-3. doi: 10.1016/s1086-5802(16)31036-1. J Am Pharm Assoc (Wash). 2000. PMID: 10665250 Review.
-
Pantoprazole: an update of its pharmacological properties and therapeutic use in the management of acid-related disorders.Drugs. 2003;63(1):101-33. doi: 10.2165/00003495-200363010-00006. Drugs. 2003. PMID: 12487624 Review.
-
Replacement of oral proton pump inhibitors with intravenous pantoprazole to effectively control gastric acid hypersecretion in patients with Zollinger-Ellison syndrome.Am J Gastroenterol. 2001 Dec;96(12):3274-80. doi: 10.1111/j.1572-0241.2001.05325.x. Am J Gastroenterol. 2001. PMID: 11774936
-
Pharmacokinetic optimisation in the treatment of gastro-oesophageal reflux disease.Clin Pharmacokinet. 1996 Nov;31(5):386-406. doi: 10.2165/00003088-199631050-00005. Clin Pharmacokinet. 1996. PMID: 9118586 Review.
-
Switching between intravenous and oral pantoprazole.J Clin Gastroenterol. 2001 Jan;32(1):27-32. doi: 10.1097/00004836-200101000-00007. J Clin Gastroenterol. 2001. PMID: 11154164 Free PMC article. Review.
Cited by
-
Intravenous pantoprazole utilization in a level 1 trauma center.Surg Endosc. 2008 Apr;22(4):967-73. doi: 10.1007/s00464-007-9531-2. Epub 2007 Aug 21. Surg Endosc. 2008. PMID: 17710489
-
Optimal treatment of Zollinger-Ellison syndrome and related conditions in elderly patients.Drugs Aging. 2003;20(14):1019-34. doi: 10.2165/00002512-200320140-00002. Drugs Aging. 2003. PMID: 14651442 Review.
-
Bleeding Meckel's Diverticulum in a 33-Year-Old Female Diagnosed with Video Capsule Endoscopy and a Technetium-99 m Pertechnetate Scan with a Favorable Response to H2 Blocker and PPI.Case Rep Gastrointest Med. 2021 Dec 9;2021:1381395. doi: 10.1155/2021/1381395. eCollection 2021. Case Rep Gastrointest Med. 2021. PMID: 34925925 Free PMC article.
-
Use of intravenous proton-pump inhibitors in a teaching hospital practice.Dig Dis Sci. 2009 Sep;54(9):1947-52. doi: 10.1007/s10620-008-0568-4. Epub 2008 Nov 26. Dig Dis Sci. 2009. PMID: 19034652
-
Effects of the histamine H2 receptor antagonist famotidine on the healing of colonic anastomosis in rats.Clinics (Sao Paulo). 2009;64(6):567-70. doi: 10.1590/s1807-59322009000600012. Clinics (Sao Paulo). 2009. PMID: 19578661 Free PMC article.
References
-
- Khan K: Pharmacologic treatment of hypersecretory disorders. Resident Reporter 2000; 5:23–28
-
- Wolfe MM, Sachs G: Acid suppression: Optimizing therapy for gastroduodenal healing, gastroesophageal reflux disease, and stress-related erosive syndrome. Gastroenterology 2000; 118:S9–S31 - PubMed
-
- Hatlebakk JG, Katz PO, Kuo B, et al.: Nocturnal gastric acidity and acid breakthrough on different regimens of omeprazole 40 mg daily. Aliment Pharmacol Ther 1998; 12: 1235–1240 - PubMed
-
- Katz PO, Anderson C, Khoury R, et al.: Gastro-oesophageal reflux associated with nocturnal gastric acid breakthrough on proton pump inhibitors. Aliment Pharmacol Ther 1998; 12:1231–1234 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
