

Tracheal gas insufflation for the prevention of morbidity and mortality in mechanically ventilated newborn infants
- PMID: 12076462
- PMCID: PMC8989411
- DOI: 10.1002/14651858.CD002973
Tracheal gas insufflation for the prevention of morbidity and mortality in mechanically ventilated newborn infants
Abstract
Background: Tracheal gas insufflation (TGI) is a technique where a continuous flow of gas is instilled into the lower trachea during conventional mechanical ventilation. TGI can improve carbon dioxide removal with lower ventilation pressures and smaller tidal volumes, potentially decreasing secondary lung injury and chronic lung disease (CLD).
Objectives: To assess whether, in mechanically ventilated neonates, the use of tracheal gas insufflation reduces mortality, CLD and other adverse clinical outcomes without significant side effects.
Search strategy: Searches were made of MEDLINE 1966 to December 2001, CINAHL 1982 to December 2001, the Cochrane Controlled Trials Register (Cochrane Library, Issue 4, 2001) and conference and symposia proceedings.
Selection criteria: Randomised controlled trials (RCT) that include newborn infants who are mechanically ventilated, and compare TGI during conventional mechanical ventilation (CMV) with CMV alone. Primary outcomes - mortality, CLD and neurodevelopmental outcome; secondary outcomes - air leak, intraventricular haemorrhage, periventricular leukomalacia, duration of mechanical ventilation, duration of respiratory support, duration of oxygen therapy, duration of hospital stay, retinopathy of prematurity, immediate adverse effects.
Data collection and analysis: Each reviewer assessed eligibility, trial quality and extracted data separately. Study authors were contacted for additional information if necessary.
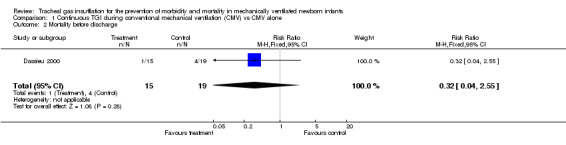
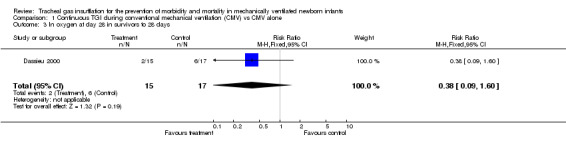
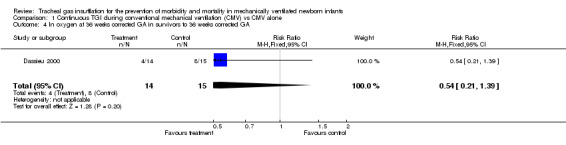
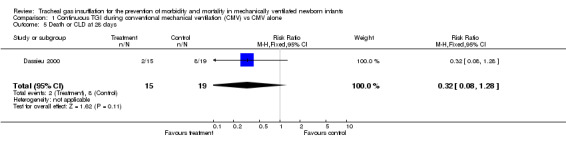
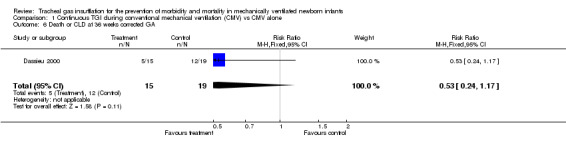
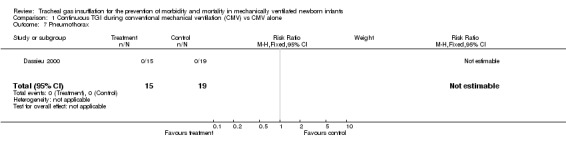
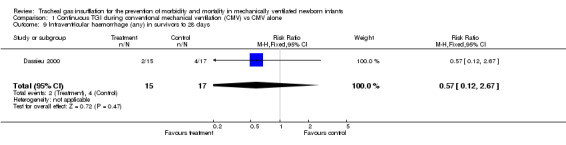
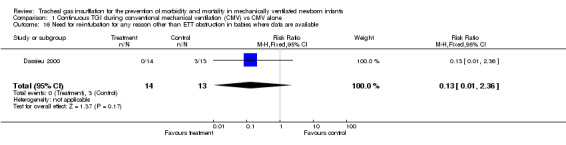
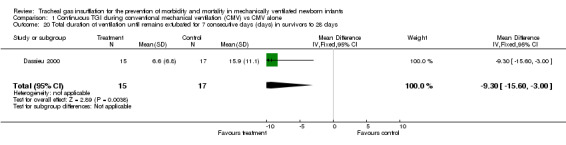
Main results: Only one small study was found to be eligible. This study found no evidence of effect on mortality, CLD or age at first extubation. The total duration of ventilation was 9.3 days shorter in the TGI group (95% CI from 15.7 to 2.9 days shorter). The age at complete weaning from ventilation was 26 days shorter in the TGI group (95% CI from 46 to 6 days shorter). There was no evidence of effect on the total duration of respiratory support, oxygen therapy or hospital stay.
Reviewer's conclusions: There is evidence from a single RCT that TGI may reduce the duration of mechanical ventilation in preterm infants - although the data from this small study do not give sufficient evidence to support the introduction of TGI into clinical practice. The technical requirements for performing TGI (as performed in the single included study) are great. There is no statistically significant reduction in the total duration of respiratory support or hospital stay. TGI cannot be recommended for general use at this time.
Conflict of interest statement
Nil
Figures















Similar articles
-
Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Cochrane Database Syst Rev. 2001;(3):CD000104. doi: 10.1002/14651858.CD000104. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2003;(1):CD000104. doi: 10.1002/14651858.CD000104. PMID: 11686950 Updated.
-
Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Cochrane Database Syst Rev. 2003;(4):CD000104. doi: 10.1002/14651858.CD000104. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2007 Jul 18;(3):CD000104. doi: 10.1002/14651858.CD000104.pub2. PMID: 14583909 Updated.
-
Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Cochrane Database Syst Rev. 2000;(2):CD000104. doi: 10.1002/14651858.CD000104. Cochrane Database Syst Rev. 2000. Update in: Cochrane Database Syst Rev. 2001;(3):CD000104. doi: 10.1002/14651858.CD000104. PMID: 10796129 Updated.
-
Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Cochrane Database Syst Rev. 2007 Jul 18;(3):CD000104. doi: 10.1002/14651858.CD000104.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2009 Jul 08;(3):CD000104. doi: 10.1002/14651858.CD000104.pub3. PMID: 17636590 Updated.
-
Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants.Cochrane Database Syst Rev. 2003;(1):CD000104. doi: 10.1002/14651858.CD000104. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2003;(4):CD000104. doi: 10.1002/14651858.CD000104. PMID: 12535383 Updated.
Cited by
-
Dead-space washout by split-flow ventilation. A new method to reduce ventilation needs in premature infants.Intensive Care Med. 2005 May;31(5):674-9. doi: 10.1007/s00134-005-2611-7. Epub 2005 Apr 19. Intensive Care Med. 2005. PMID: 15838679 Clinical Trial.
-
Dead space reduction by Kolobow's endotracheal tube does not justify the waiving of volume monitoring in small, ventilated lungs.J Clin Monit Comput. 2014 Dec;28(6):605-11. doi: 10.1007/s10877-014-9559-5. Epub 2014 Jan 28. J Clin Monit Comput. 2014. PMID: 24469384
-
Effect of the Y-piece of the ventilation circuit on ventilation requirements in extremely low birth weight infants.Intensive Care Med. 2005 Aug;31(8):1095-100. doi: 10.1007/s00134-005-2711-4. Epub 2005 Jul 6. Intensive Care Med. 2005. PMID: 15999252
References
References to studies included in this review
Dassieu 2000 {published data only}
-
- Dassieu G, Brochard L, Benani M, Avenel S, Danan C. Continuous tracheal gas insufflation in preterm infants with hyaline membrane disease. American Journal of Respiratory and Critical Care Medicine 2000;162:826‐31. - PubMed
References to studies excluded from this review
Wald 2005 {published data only}
-
- Wald M, Kalous P, Lawrenz K, Jeitler V, Weninger M, Kirchner L. Dead‐space washout by split‐flow ventilation. A new method to reduce ventilation needs in premature infants. Intensive Care Medicine 2005;31:674. - PubMed
Additional references
Bernath 1997
-
- Bernath MA, Henning R. Tracheal gas insufflation reduces requirements for mechanical ventilation in a rabbit model of respiratory distress syndrome. Anaesthesia and Intensive Care 1997;25:15‐22. - PubMed
Danan 1996
-
- Danan C, Dassieu G, Janaud J‐C, Brochard L. Efficacy of dead‐space washout in mechanically ventilated premature newborns. American Journal of Respiratory and Critical Care Medicine 1996;153:1571‐6. - PubMed
Dassieu 1998
-
- Dassieu G, Brochard L, Agudze E, Patkai J, Janaud J‐C, Danan C. Continuous tracheal gas insufflation enables a volume reduction strategy in hyaline membrane disease: technical aspects and clinical results. Intensive Care Medicine 1998;24:1076‐82. - PubMed
De Robertis 1999
-
- Robertis E, Sigurdsson SE, Drefeldt B, Jonson B. Aspiration of airway dead space. A new method to enhance CO2 elimination. American Journal of Respiratory and Critical Care Medicine 1999;159:728‐32. - PubMed
Richecoeur 1999
-
- Richecoeur J, Lu Q, Vieira SRR, Puybasset L, Kalfon P, Coriat P, Rouby J‐J. Expiratory washout versus optimization of mechanical ventilation during permissive hypercapnia in patients with severe acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine 1999;160:77‐85. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources