

Cognitive slowing in Parkinson's disease: a behavioral evaluation independent of motor slowing
- PMID: 12077214
- PMCID: PMC6757751
- DOI: 10.1523/JNEUROSCI.22-12-05198.2002
Cognitive slowing in Parkinson's disease: a behavioral evaluation independent of motor slowing
Abstract
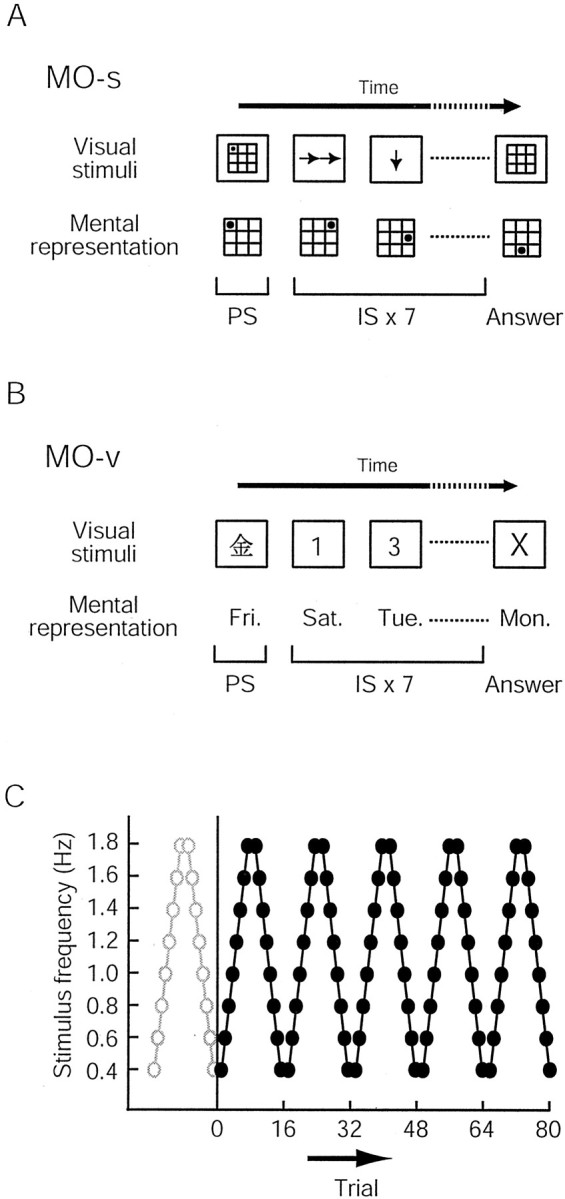
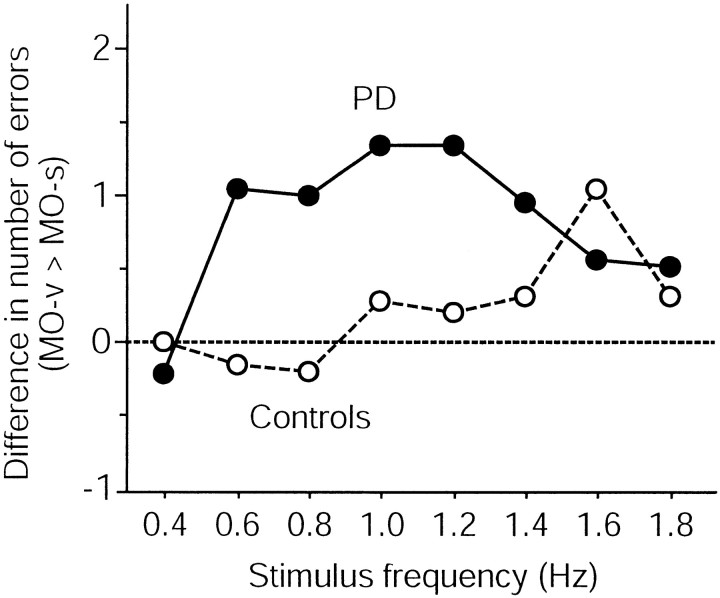
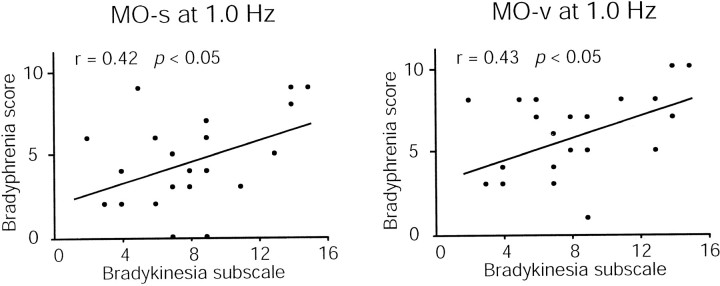
Parkinson's disease (PD) is attributable primarily to depletion of dopamine in the basal ganglia, but the full effects of this depletion are unknown. It is well known that PD involves motor slowing, and although it is not easy to distinguish between the motor and cognitive components of behavior, clinical observations suggest that cognitive processing may also be compromised. However, it remains unclear whether such cognitive involvement exists, and if so, to what extent. Previous studies of cognitive slowing in PD have yielded conflicting results. This may be attributable to variations in experimental procedures, because most of the experiments used reaction-time tasks, which are inevitably confounded by motor components. In the present study, we evaluated the speed of cognitive processing in patients with PD without bradykinesia as a variable. We developed a mental-operation task that required serial updating of mental representations in response to a series of visual stimuli. By changing the speed of visual presentation and evaluating performance accuracy, the speed of cognitive processing was assessed independently of motor slowing. Cognitive impairment in PD became evident when higher speeds of cognitive processing (verbal more so than spatial) were required. In addition, cognitive slowing and motor slowing were significantly correlated. The results of the present study suggest that slowing in PD is not restricted to the motor domain but can be generally observed in other domains of behavior, including cognitive mental operations.
Figures

References
-
- Agostino R, Berardelli A, Formica A, Accornero N, Manfredi M. Sequential arm movements in patients with Parkinson's disease, Huntington's disease and dystonia. Brain. 1992;115:1481–1495. - PubMed
-
- Benecke R, Rothwell JC, Dick JP, Day BL, Marsden CD. Performance of simultaneous movements in patients with Parkinson's disease. Brain. 1986;109:739–757. - PubMed
-
- Benecke R, Rothwell JC, Dick JP, Day BL, Marsden CD. Disturbance of sequential movements in patients with Parkinson's disease. Brain. 1987;110:361–379. - PubMed
-
- Berry EL, Nicolson RI, Foster JK, Behrmann M, Sagar HJ. Slowing of reaction time in Parkinson's disease: the involvement of the frontal lobes. Neuropsychologia. 1999;37:787–795. - PubMed
-
- Boecker H, Dagher A, Ceballos-Baumann AO, Passingham RE, Samuel M, Friston KJ, Poline J, Dettmers C, Conrad B, Brooks DJ. Role of the human rostral supplementary motor area and the basal ganglia in motor sequence control: investigations with H2 15O PET. J Neurophysiol. 1998;79:1070–1080. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical