

Retinal nerve fibre layer loss in patients with type 1 diabetes mellitus without retinopathy
- PMID: 12084737
- PMCID: PMC1771182
- DOI: 10.1136/bjo.86.7.725
Retinal nerve fibre layer loss in patients with type 1 diabetes mellitus without retinopathy
Abstract
Background/aim: There is evidence suggesting the occurrence of neurovisual abnormalities in patients with diabetes without retinopathy. However, the determination of abnormalities in the neural and glial elements in vivo is difficult. The aim of this study was to investigate whether a retinal nerve fibre layer (RNFL) defect (as determined by scanning laser polarimetry, SLP) is present in patients without clinical manifestations of diabetic retinopathy.
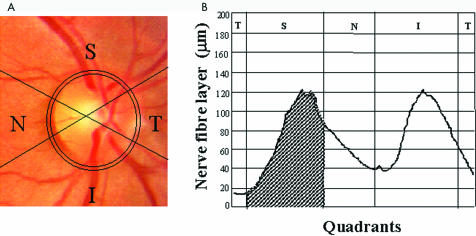
Methods: 12 patients with type 1 diabetes mellitus (DM) without retinopathy or other diabetes induced microvascular complications, underwent a complete ophthalmological examination, including automated perimetry and RNFL measurements with a nerve fibre layer analyser GDx. The data were compared with a normal control group matched for age and sex.
Results: The superior segment retardation in patients with diabetes was lower than in the control group, based on the superior integral (0.19 (SD 0.06) v 0.23 (0.04) mm(2), p=0.03) and the superior average (71.0 (11.05) v 84.27 (10.56) microm, p=0.007) parameters.
Conclusion: This finding may be indicative of significant nerve fibre loss in the superior segment of the retina in patients with type 1 diabetes mellitus but without retinopathy. The meaning of intraretinal differences in RNFL retardation, indicating asymmetric NFL loss, in patients with diabetes is yet not understood.
Figures

Comment in
-
Retinal nerve fibre layer loss in diabetes mellitus without retinopathy.Br J Ophthalmol. 2002 Jul;86(7):709. doi: 10.1136/bjo.86.7.709. Br J Ophthalmol. 2002. PMID: 12084732 Free PMC article. No abstract available.
References
-
- Kuwabara T, Cogan DG. Retinal vascular patterns. VI. Mural cells of retinal capillaries. Arch Ophthalmol 1963;69:492–502. - PubMed
-
- Frank RN. On the pathogenesis of diabetic retinopathy. Ophthalmology 1984;91:626–34. - PubMed
-
- Hyvrinen L, Laurinen P, Rovano J. Contrast sensitivity in evaluation of visual impairment due to diabetes. Acta Ophthalmol 1983;61:94–101. - PubMed
-
- Dosso AA, Bonvin ER, Morel Y, et al. Risk factors associated with contrast sensitivity loss in diabetic patients. Graefes Arch Clin Exp Ophthalmol 1996;234:300–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical