

A randomised, prospective study comparing trabeculectomy augmented with antimetabolites with a viscocanalostomy technique for the management of open angle glaucoma uncontrolled by medical therapy
- PMID: 12084743
- PMCID: PMC1771200
- DOI: 10.1136/bjo.86.7.748
A randomised, prospective study comparing trabeculectomy augmented with antimetabolites with a viscocanalostomy technique for the management of open angle glaucoma uncontrolled by medical therapy
Abstract
Aims: To compare trabeculectomy with viscocanalostomy for the control of intraocular pressure (IOP) in open angle glaucoma (OAG) uncontrolled by medical therapy.
Methods: 48 patients (50 eyes) with uncontrolled OAG were randomised to either trabeculectomy (25 eyes) or a viscocanalostomy technique (25 eyes). Preoperatively, eyes were graded in terms of risk factors for drainage failure. Those undergoing trabeculectomy were given intraoperative antimetabolites (5-fluorouracil 25 mg/ml (5-FU), mitomycin C (MMC) 0.2 mg/ml and 0.4 mg/ml) according to a standard protocol. Antimetabolites were not used intraoperatively in eyes undergoing viscocanalostomy, but they were randomised to the use of viscoelastic (Healonid GV) for intraoperative intracanalicular injection.
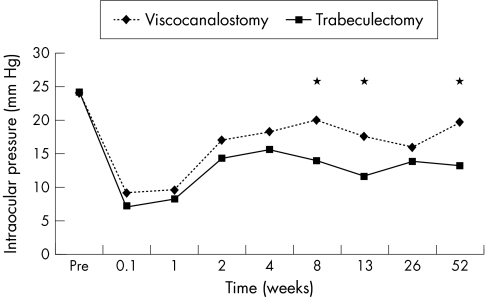
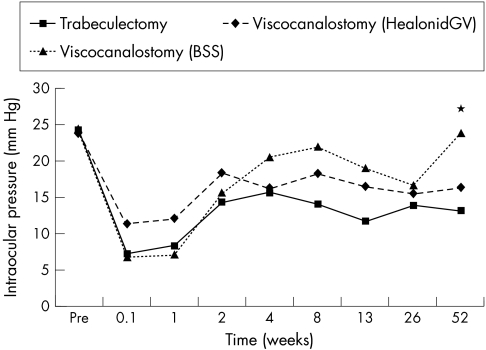
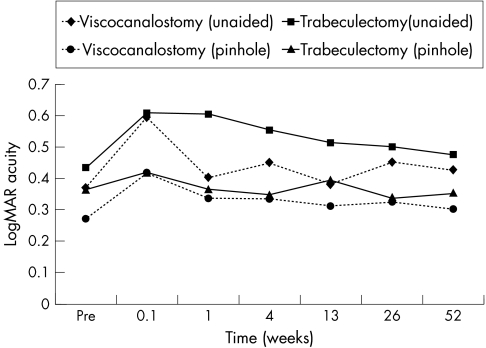
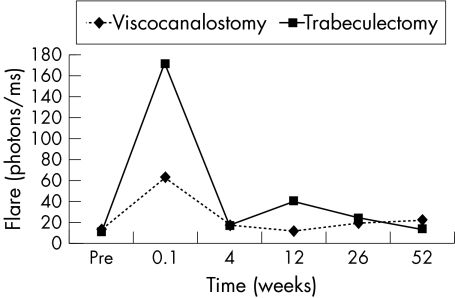
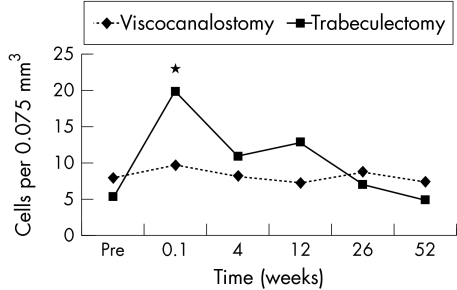
Results: There were no significant differences between the groups in age, sex, type of OAG, preoperative medications, risk factors for drainage failure, and preoperative IOP. Mean follow up was 19 months (range 6-24 months). It was 12 months or longer in all eyes, except one lost to follow up at 6 months. At 12 months, complete success (IOP <21 mm Hg without antiglaucoma medications) was seen in all eyes undergoing trabeculectomy (100%), but in only 64% of eyes undergoing viscocanalostomy (p<0.001). The mean IOP was lower at 12 months (p<0.001) with trabeculectomy and the number of eyes with IOPs of 15 mm Hg or less was greater (p<0.05). The mean IOP at 12 months was lower in eyes that had undergone viscocanalostomy using intraoperative intracanalicular Healonid GV injection compared to those where only balanced saline solution had been used (p<0.01). However, in terms of complete success there was no difference between the viscocanalostomy groups (p<0.1). With the exception of measurements at 1 week, visual recovery (logMAR acuity) was similar and laser flare and cell values showed little differences between the groups. Corneal topography and keratometry at 12 months were little different from preoperative values. Postoperative interventions (subconjunctival 5-FU and needling procedures) were similar between the groups. Transient complications such as early bleb leak and hyphaema were more common in the trabeculectomy group (p<0.05). Postoperative cataract formation was more common after trabeculectomy (p<0.05).
Conclusions: IOP control appears to be better with trabeculectomy. Viscocanalostomy is associated with fewer postoperative complications, although significant complications permanently impairing vision did not occur with either technique.
Figures
Comment in
-
Surgery for glaucoma in the 21st century.Br J Ophthalmol. 2002 Jul;86(7):710-1. doi: 10.1136/bjo.86.7.710. Br J Ophthalmol. 2002. PMID: 12084733 Free PMC article. No abstract available.
-
Trabeculectomy augmented with antimetabolites with a viscocanalostomy technique for the management of open angle glaucoma.Br J Ophthalmol. 2003 Mar;87(3):374-5. doi: 10.1136/bjo.87.3.374-a. Br J Ophthalmol. 2003. PMID: 12598471 Free PMC article. No abstract available.
-
Surgery for glaucoma.Br J Ophthalmol. 2003 Apr;87(4):517. doi: 10.1136/bjo.87.4.517. Br J Ophthalmol. 2003. PMID: 12642338 Free PMC article. No abstract available.
References
-
- Sugar HS. Experimental trabeculectomy in glaucoma. Am J Ophthalmol 1961;51:623.
-
- Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol 1968;66:673–9. - PubMed
-
- Cairns JE. Surgical treatment of primary open-angle glaucoma. Trans Ophthalmol Soc UK 1972;92:745–56. - PubMed
-
- Watson PG, Barrett F. Effectiveness of trabeculectomy in glaucoma. Am J Ophthalmol 1975;79:831–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources