

The efficacy of metallic stent placement in the treatment of colorectal obstruction
- PMID: 12087197
- PMCID: PMC2713840
- DOI: 10.3348/kjr.2002.3.2.79
The efficacy of metallic stent placement in the treatment of colorectal obstruction
Abstract
Objective: To evaluate the efficacy of newly designed covered and non-covered coated colorectal stents for colonic decompression.
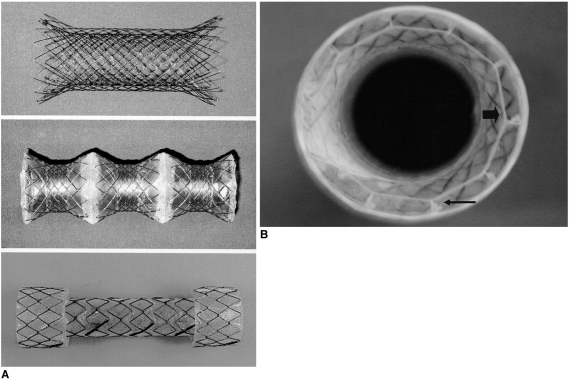
Materials and methods: Twenty-six patients, (15 palliative cases and 11 preoperative) underwent treatment for the relief of colorectal obstruction using metallic stents positioned under fluoroscopic guidance. In 24 of the 26, primary colorectal carcinoma was diagnosed, and in the remaining two, recurrent colorectal carcinoma. Twenty-one patients were randomly selected to receive either a type A or type B stent; for the remaining five, type C was used. Type A, an uncovered nitinol wire stent, was lightly coated to ensure structural integrity. Type B (flare type) and C (shoulder type) stents were polyurethane covered and their diameter was 24 and 26 mm, respectively. The rates of technical success, clinical success, and complications were analyzed using the chi-square test, and to analyse the mean period of patency, the Kaplan-Meier method was used.
Results: Thirty of 31 attempted placements in 26 patients were successful, with a technical success rate of 96.8% (30/31) and a clinical success rate of 80.0% (24/30). After clinically successful stent placement, bowel decompression occurred within 1-4 (mean, 1.58+/-0.9) days. Five of six clinical failures involved stent migration and one stent did not expand after successful placement. In the preoperative group, 11 stents, one of which migrated, were placed in ten patients, in all of whom bowel preparation was successful. In the palliative group, 19 stents were placed in 15 patients. The mean period of patency was 96.25+/-105.12 days: 146.25+/-112.93 for type-A, 78.82+/-112.26 for type-B, and 94.25+/-84.21 for type-C. Complications associated with this procedure were migration (n=6, 20%), pain (n=4, 13.3%), minor bleeding (n=5, 16.7%), incomplete expansion (n=1, 3.3%), and tumor ingrowth (n=1, 3.3%). The migration rate was significantly higher in the type-B group than in other groups (p=0.038).
Conclusion: Newly designed covered and non-covered metallic stents of a larger diameter are effective for the treatment of colorectal obstruction. The migration rate of covered stents with flaring is higher than that of other types. For evaluation of the ideal stent configuration for the relief of colorectal obstruction, a clinical study involving a larger patient group is warranted.
Figures



Similar articles
-
Malignant colorectal obstruction: treatment with a flexible covered stent.Radiology. 1998 Feb;206(2):415-21. doi: 10.1148/radiology.206.2.9457194. Radiology. 1998. PMID: 9457194
-
Radiologic placement of uncovered stents for the treatment of malignant colorectal obstruction.J Vasc Interv Radiol. 2010 Aug;21(8):1244-9. doi: 10.1016/j.jvir.2010.04.009. Epub 2010 Jul 3. J Vasc Interv Radiol. 2010. PMID: 20598564
-
Fluoroscopically guided placement of self-expandable metallic stents and stent-grafts in the treatment of acute malignant colorectal obstruction.J Vasc Interv Radiol. 2008 Dec;19(12):1709-16. doi: 10.1016/j.jvir.2008.08.020. Epub 2008 Oct 8. J Vasc Interv Radiol. 2008. PMID: 18845454
-
[Treatement of colorectal obstruction with self-expanding metallic stents under fluoroscopic guidance].J Radiol. 2002 Apr;83(4 Pt 1):473-7. J Radiol. 2002. PMID: 12045744 Review. French.
-
Advances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents.Radiology. 2000 Jun;215(3):659-69. doi: 10.1148/radiology.215.3.r00jn30659. Radiology. 2000. PMID: 10831681 Review.
Cited by
-
Usefulness of multifunctional gastrointestinal coil catheter for colorectal stent placement.Eur Radiol. 2008 Nov;18(11):2530-4. doi: 10.1007/s00330-008-1042-6. Epub 2008 Jun 4. Eur Radiol. 2008. PMID: 18523778
-
Interventional management of malignant colorectal obstruction: use of covered and uncovered stents.Korean J Radiol. 2007 Jan-Feb;8(1):57-63. doi: 10.3348/kjr.2007.8.1.57. Korean J Radiol. 2007. PMID: 17277564 Free PMC article.
-
A temporary self-expanding metallic stent for malignant colorectal obstruction.World J Gastroenterol. 2013 Feb 21;19(7):1119-23. doi: 10.3748/wjg.v19.i7.1119. World J Gastroenterol. 2013. PMID: 23467379 Free PMC article.
-
Stents for colorectal obstruction: Past, present, and future.World J Gastroenterol. 2016 Jan 14;22(2):842-52. doi: 10.3748/wjg.v22.i2.842. World J Gastroenterol. 2016. PMID: 26811630 Free PMC article. Review.
-
Palliative stent implantation in the treatment of malignant colorectal obstruction.Surg Endosc. 2006 Jun;20(6):909-14. doi: 10.1007/s00464-005-0594-7. Epub 2006 May 11. Surg Endosc. 2006. PMID: 16738981
References
-
- Camunez F, Echenagusia A, Simo G, Turegano F, Vazquez J, Barreiro-Meiro I. Malignant colorectal obstruction treated by means of self-expanding metallic stents: Effectiveness before surgery and in palliation. Radiology. 2000;216:492–497. - PubMed
-
- Mainar A, Ariza MADG, Tejero E, et al. Acute colorectal obstruction treatment with self-expandable metallic stents before scheduled surgery: results of a multicenter study. Radiology. 1999;210:65–69. - PubMed
-
- De Gregorio MA, Mainar A, Tejero E, et al. Acute colorectal obstruction: stent placement for palliative treatment: results of a multicenter study. Radiology. 1998;209:117–120. - PubMed
-
- Saida Y, Sumiyama Y, Narao J, Takase M. Stent endoprosthesis for obstructive colorectal cancers. Dis Colon Rectum. 1996;39:552–555. - PubMed
-
- Loggie BW. Surgical concept in the treatment of colorectal cancer. Semin Roentgenol. 1996;31:111–117. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
