

Posthaemorrhagic ventricular dilatation in the premature infant: natural history and predictors of outcome
- PMID: 12091289
- PMCID: PMC1721419
- DOI: 10.1136/fn.87.1.f37
Posthaemorrhagic ventricular dilatation in the premature infant: natural history and predictors of outcome
Abstract
Objective: To investigate the natural history and predictors of outcome of posthaemorrhagic ventriculomegaly in the very low birthweight (VLBW) infant.
Methods: All VLBW infants admitted between September 1994 and September 1997 to the neonatal intensive care units of Brigham and Women's Hospital (Boston), Children's Hospital (Boston), and Christchurch Women's Hospital (New Zealand) with germinal matrix intraventricular haemorrhage (IVH) were identified. All charts and ultrasound scans were reviewed to define the natural history and perinatal and/or postnatal factors of value in prediction of the course of posthaemorrhagic ventriculomegaly. Progressive ventricular dilatation (PVD) was defined from the results of serial cranial ultrasound scans.
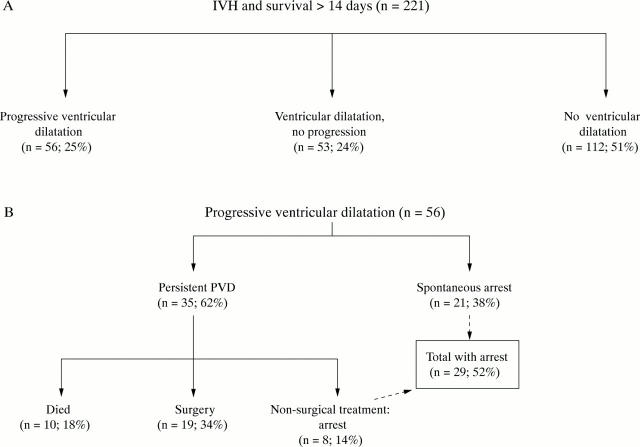
Results: A total of 248 VLBW infants had evidence of IVH (22% of all VLBW infants, mean (SD) gestational age 26.8 (2.6) weeks). A quarter of the infants exhibited PVD. Spontaneous arrest of PVD occurred without treatment in 38% of infants with PVD. Of the remaining 62% with persistent PVD, 48% received non-surgical treatment only (pharmacological and/or drainage of cerebrospinal fluid by serial lumbar punctures), 34% received surgical treatment with insertion of a ventriculoperitoneal reservoir and/or shunt, and 18% died. The development of PVD after IVH and adverse short term outcome, such as the requirement for surgery, were predicted most strongly by the severity of IVH.
Conclusions: These data reflect the natural history of PVD in the 1990s and show that, despite a slight reduction in its overall incidence, there appears to be a more aggressive course, with appreciable mortality and morbidity in the extremely premature infant. The major predictor of adverse short term outcome, defined as death or need for surgical intervention, was the severity of IVH. These findings may be valuable for the management of very small premature infants.
Figures
Comment in
-
Progressive ventricular dilatation (PVD) over the past 22 years.Arch Dis Child Fetal Neonatal Ed. 2003 May;88(3):F257. doi: 10.1136/fn.88.3.f257-a. Arch Dis Child Fetal Neonatal Ed. 2003. PMID: 12719408 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources