

Opposite effects of cyclooxygenase-1 and -2 activity on the pressor response to angiotensin II
- PMID: 12093889
- PMCID: PMC151026
- DOI: 10.1172/JCI14752
Opposite effects of cyclooxygenase-1 and -2 activity on the pressor response to angiotensin II
Erratum in
- J Clin Invest 2002 Aug;110(3):419
Abstract
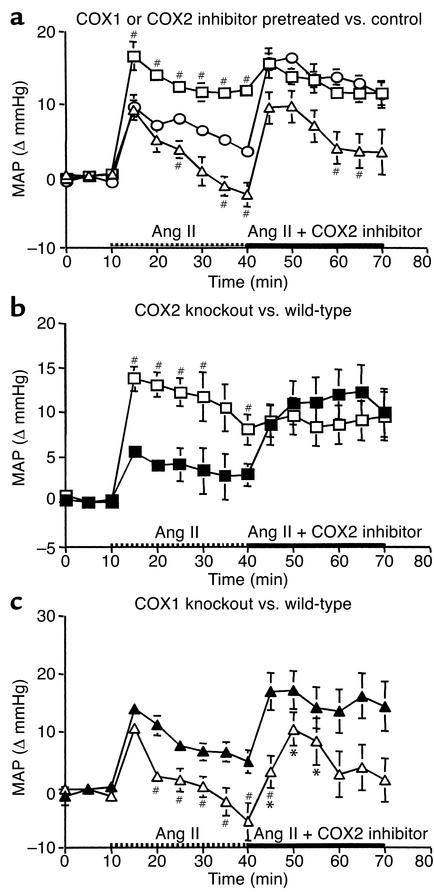
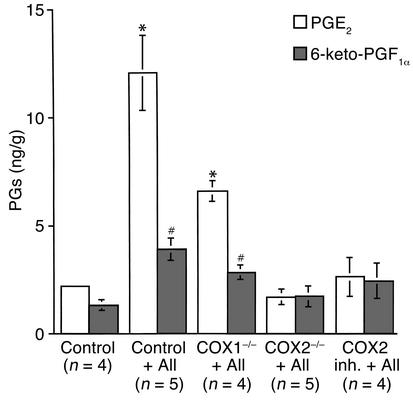
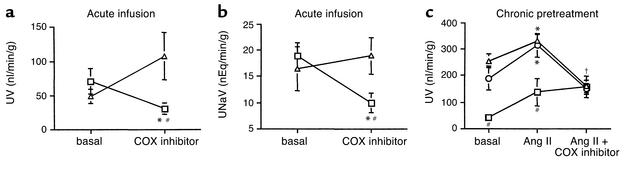
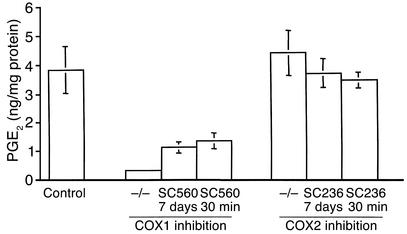
Therapeutic use of cyclooxygenase-inhibiting (COX-inhibiting) nonsteroidal antiinflammatory drugs (NSAIDs) is often complicated by renal side effects including hypertension and edema. The present studies were undertaken to elucidate the roles of COX1 and COX2 in regulating blood pressure and renal function. COX2 inhibitors or gene knockout dramatically augment the pressor effect of angiotensin II (Ang II). Unexpectedly, after a brief increase, the pressor effect of Ang II was abolished by COX1 deficiency (either inhibitor or knockout). Ang II infusion also reduced medullary blood flow in COX2-deficient but not in control or COX1-deficient animals, suggesting synthesis of COX2-dependent vasodilators in the renal medulla. Consistent with this, Ang II failed to stimulate renal medullary prostaglandin E(2) and prostaglandin I(2) production in COX2-deficient animals. Ang II infusion normally promotes natriuresis and diuresis, but COX2 deficiency blocked this effect. Thus, COX1 and COX2 exert opposite effects on systemic blood pressure and renal function. COX2 inhibitors reduce renal medullary blood flow, decrease urine flow, and enhance the pressor effect of Ang II. In contrast, the pressor effect of Ang II is blunted by COX1 inhibition. These results suggest that, rather than having similar cardiovascular effects, the activities of COX1 and COX2 are functionally antagonistic.
Figures

Comment in
-
The choreography of cyclooxygenases in the kidney.J Clin Invest. 2002 Jul;110(1):33-4. doi: 10.1172/JCI16044. J Clin Invest. 2002. PMID: 12093885 Free PMC article. Review. No abstract available.
References
-
- FitzGerald GA, Patrono C. The coxibs, selective inhibitors of cyclooxygenase-2. N Engl J Med. 2001;345:433–442. - PubMed
-
- Breyer MD, Harris RC. Cyclooxygenase 2 and the kidney. Curr Opin Nephrol Hypertens. 2001;10:89–98. - PubMed
-
- Whelton A, et al. Cyclooxygenase-2-specific inhibitors and cardiorenal function: a randomized, controlled trial of celecoxib and rofecoxib in older hypertensive osteoarthritis patients. Am J Ther. 2001;8:85–95. - PubMed
-
- Page J, Henry D. Consumption of NSAIDs and the development of congestive heart failure in elderly patients: an underrecognized public health problem. Arch Intern Med. 2000;160:777–784. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
