

B lymphocytopenia in rheumatoid arthritis is associated with the DRB1 shared epitope and increased acute phase response
- PMID: 12106500
- PMCID: PMC125293
- DOI: 10.1186/ar420
B lymphocytopenia in rheumatoid arthritis is associated with the DRB1 shared epitope and increased acute phase response
Abstract
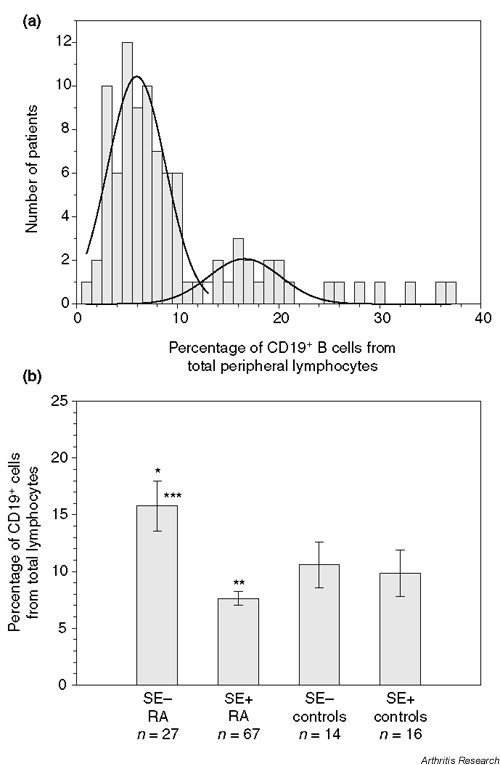
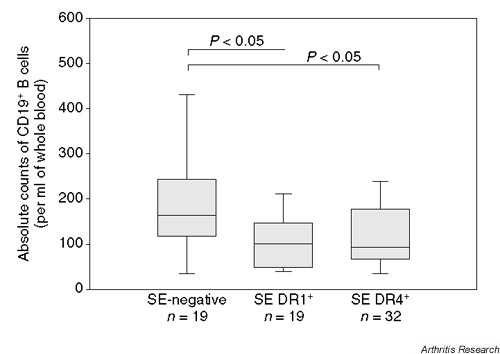
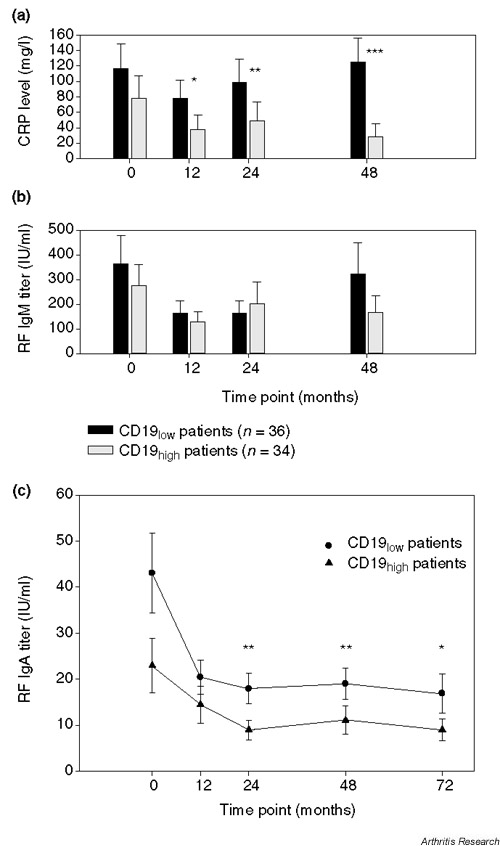
The influence of HLA DRB1 alleles on B-cell homeostasis was analyzed in 164 patients with rheumatoid arthritis (RA). The percentages of CD19+ B lymphocytes determined in the peripheral circulation of 94 retrospectively recruited RA patients followed a bimodal distribution. Two frequency peaks (B-cell(low) patients and B-cell(high) patients) were separated by the population median of a B-cell frequency of 8.5% of all lymphocytes. Human leucocyte antigen genotyping revealed that the B-cell(low) patients were more frequently positive for the RA-associated HLA DRB1 shared epitope (SE) than were B-cell(high) patients. Accordingly, SE-positive patients had lower CD19 percentages in the rank-sum analysis when compared with SE-negative patients, and were markedly B lymphocytopenic when compared with a healthy control group. To confirm the differential frequencies of CD19+ B cells, absolute numbers in peripheral blood were determined prospectively in a cohort of 70 RA patients with recent onset disease. SE-positive patients were found to have lower absolute numbers of circulating CD19+ B cells. B-cell counts below the mean of the study population were associated with higher acute phase response and with increased levels of rheumatoid factor IgA. No correlation between absolute numbers of circulating B cells and radiographic progression of joint destruction was seen. The influence of immunogenetic parameters on B-cell homeostasis in RA reported here has not been described previously. The clinical relevance of B lymphocytopenia in SE-positive RA will be further investigated in longitudinal studies.
Figures
References
-
- Juby A, Johnston C, Davis P, Russell AS. Antinuclear and antineutrophil cytoplasmic antibodies (ANCA) in the sera of patients with Felty's syndrome. Br J Rheumatol. 1992;31:185–188. - PubMed
-
- Rother E, Metzger D, Lang B, Melchers I, Peter HH. Anti-neutrophil cytoplasm antibodies (ANCA) in rheumatoid arthritis: relationship to HLA-DR phenotypes, rheumatoid factor, antinuclear antibodies and disease severity. Rheumatol Int. 1994;14:155–161. - PubMed
-
- Braun MG, Csernok E, Schmitt WH, Gross WL. Incidence, target antigens, and clinical implications of antineutrophil cytoplasmic antibodies in rheumatoid arthritis. J Rheumatol. 1996;23:826–830. - PubMed
-
- Charles PJ, Maini RN. Antibodies to neutrophil cytoplasmic antigens in rheumatoid arthritis. Adv Exp Med Biol. 1993;336:367–370. - PubMed
-
- Mulder AH, Horst G, van Leeuwen MA, Limburg PC, Kallenberg CG. Antineutrophil cytoplasmic antibodies in rheumatoid arthritis. Characterization and clinical correlations. Arthritis Rheum. 1993;36:1054–1060. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
