

Primary thoracoscopic evaluation of pleural effusion with local anesthesia: an alternative approach
- PMID: 12113418
- PMCID: PMC3043419
Primary thoracoscopic evaluation of pleural effusion with local anesthesia: an alternative approach
Abstract
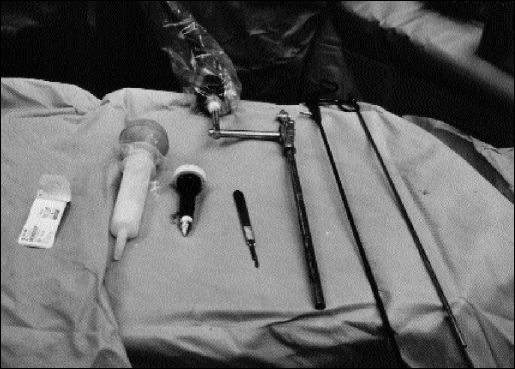
Objective: The development of a thoracoscopically assisted technique to be performed with the patient under local anesthesia for both diagnostic and therapeutic purposes when treating pleural effusions and empyemas in high-risk surgical patients.
Methods: Twenty patients with pleural effusion or empyema who were also determined to be at high risk for complications following a thoracotomy, pleural biopsy, general anesthesia, or all of these, underwent placement of a thoracoscope while under local anesthesia followed by thoracic fluid drainage, pleural biopsy, and pleurodesis as required. Patients were retrospectively evaluated for a variety of factors including personal history, pre-existing medical conditions, and pre- and postoperative course.
Results: The average age of the patients was 59 years (18 to 89) with a 55% male/45% female sex distribution. Patients had this procedure as a consequence of malignancy (50%), empyema (30%), spontaneous pneumothorax (10%), bronchiectasis (50%), or heart failure (5%). The average duration of the procedure was 62 minutes (20 to 190), with an average of 861 mL of fluid drainage, and 114 mL of estimated blood loss. The tube thoracostomy was usually removed on the sixth (0 to 13) postprocedure day. This procedure was well tolerated by the patients with the majority of pain management being achieved with patient controlled analgesia (58%). The direct complication rate was 10%, with 2 patients requiring endotracheal intubation.
Conclusion: This novel thoracoscopic procedure represents an acceptable alternative to the traditional treatment of pleural effusions and empyema with comparable outcome parameters and morbidity. This technique may eventually become the standard of care for the treatment of pleural effusions.
Figures

References
-
- Jacobaeus HC. Uber lapro-und thorakoskopie. Beitr Klin Tuberk. 1912;25:334–341
-
- Hau T, Forster E, Gandawidjaja L, Heemken R. Thoracoscopic pulmonary surgery: indications and results. Eur J Surg. 1996;162:23–28 - PubMed
-
- Saenz NC, Conlon KCP, Aronson DA, LaQuaglia MP. The application of malignancies. J Laparosc Adv Surg Tech. 1997;7(5):110–117 - PubMed
-
- Matthay RA, Coppage L, Shaw C, Fielderman AE. Malignancies metastatic to the pleura. Inves Radiol. 1990;25:601–619 - PubMed
-
- Lynch TE. Management of malignant pleural effusion. Chest. 1993;103:385S–389S - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources