

Preload-adjusted maximal power: a novel index of left ventricular contractility in atrial fibrillation
- PMID: 12117848
- PMCID: PMC1767221
- DOI: 10.1136/heart.88.2.170
Preload-adjusted maximal power: a novel index of left ventricular contractility in atrial fibrillation
Abstract
Background: Left ventricular contractility in atrial fibrillation is known to change in a beat to beat fashion, but there is no gold standard for contractility indices in atrial fibrillation, especially those measured non-invasively.
Objective: To determine whether the non-invasive index of contractility "preload-adjusted PWR(max)" (maximal ventricular power divided by the square of end diastolic volume) can accurately measure left ventricular contractility in a beat to beat fashion in atrial fibrillation.
Methods: Atrial fibrillation was induced experimentally using 60 Hz stimulation of the atrium and maintained in 12 sheep; four received diltiazem, four digoxin, and four no drugs (control). Aortic flow, left ventricular volume, and left ventricular pressure were monitored simultaneously. Preload-adjusted PWR(max), the slope of the end systolic pressure-volume relation (E(max)), and the maximum rate of change of left ventricular pressure (dP/dt(max)) were calculated in a beat to beat fashion.
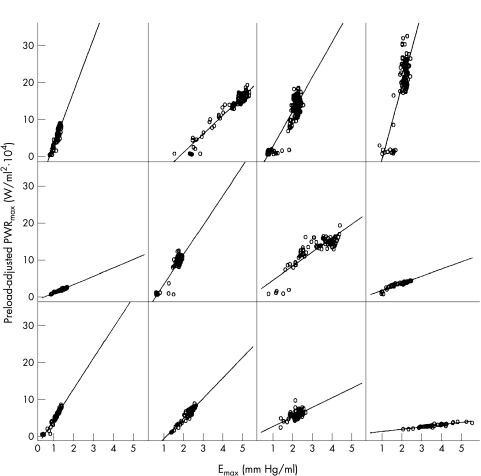
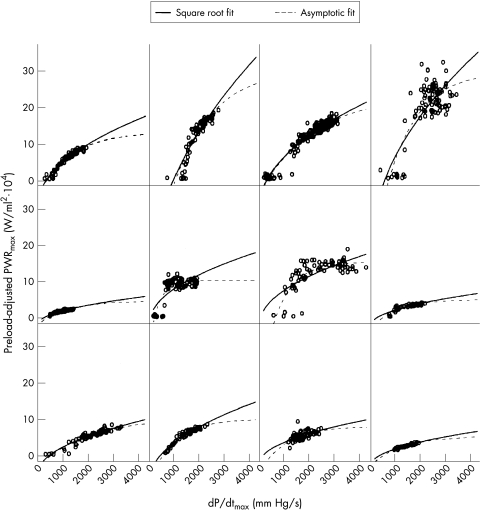
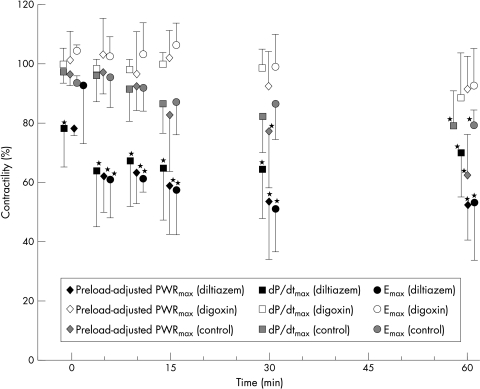
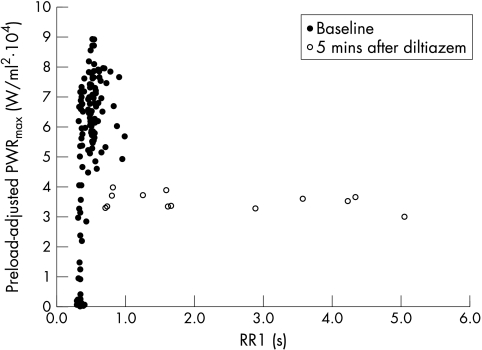
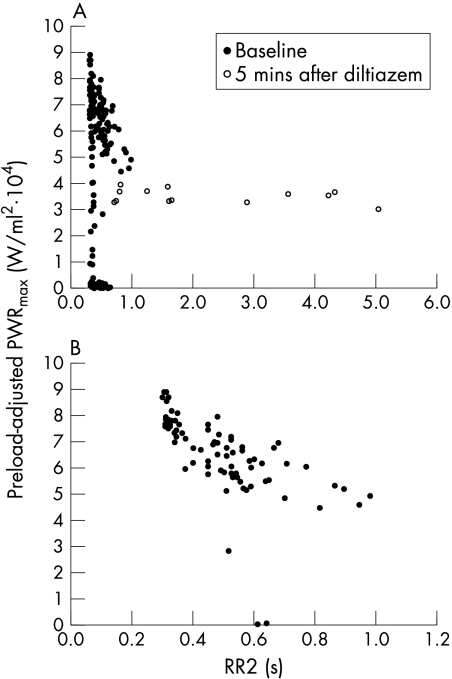
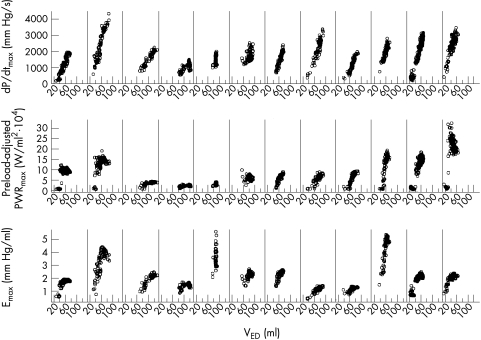
Results: Preload-adjusted PWR(max) correlated linearly with load independent E(max) (p < 0.0001) and curvilinearly with load dependent dP/dt(max) (p < 0.0001), which suggested the load independence of preload-adjusted PWR(max). After five minutes of diltiazem administration, preload-adjusted PWR(max), dP/dt(max), and E(max) fell significantly (p < 0.0001) to 62%, 64%, and 61% of baseline, respectively. Changes were not significant after five minutes of digoxin (103%, 98%, and 102%) or in controls (97%, 96%, and 95%).
Conclusions: Preload-adjusted PWR(max) correlates linearly with E(max) and is a useful measure of contractility even in atrial fibrillation. Non-invasive application of this method, in combination with echocardiography and tonometry, may yield important information for optimising the treatment of patients with atrial fibrillation.
Figures
Similar articles
-
Assessment of dsigma*/dt (max), a load independent index of contractility, in the canine.Cardiovasc Eng. 2009 Jun;9(2):49-55. doi: 10.1007/s10558-009-9073-4. Epub 2009 May 23. Cardiovasc Eng. 2009. PMID: 19466542
-
Left ventricular beat to beat performance in atrial fibrillation: dependence on contractility, preload, and afterload.Heart. 1999 Nov;82(5):575-80. doi: 10.1136/hrt.82.5.575. Heart. 1999. PMID: 10525512 Free PMC article.
-
Myocardial longitudinal peak systolic acceleration (pSac): relationship to ejection phase, pressure, and contractility.Echocardiography. 2012 May;29(5):541-53. doi: 10.1111/j.1540-8175.2011.01628.x. Epub 2012 Feb 14. Echocardiography. 2012. PMID: 22329750
-
Determinants of left ventricular preload-adjusted maximal power.Am J Physiol Heart Circ Physiol. 2003 Jun;284(6):H2295-301. doi: 10.1152/ajpheart.01110.2002. Epub 2003 Mar 13. Am J Physiol Heart Circ Physiol. 2003. PMID: 12637350
-
Myocardial contractility in the echo lab: molecular, cellular and pathophysiological basis.Cardiovasc Ultrasound. 2005 Sep 8;3:27. doi: 10.1186/1476-7120-3-27. Cardiovasc Ultrasound. 2005. PMID: 16150150 Free PMC article. Review.
Cited by
-
Sex-related changes in cardiac function following myocardial infarction in mice.Am J Physiol Regul Integr Comp Physiol. 2008 Aug;295(2):R528-34. doi: 10.1152/ajpregu.90342.2008. Epub 2008 Jun 11. Am J Physiol Regul Integr Comp Physiol. 2008. PMID: 18550865 Free PMC article.
-
Heart-protective effect of n-3 PUFA demonstrated in a rat model of diabetic cardiomyopathy.Mol Cell Biochem. 2014 Apr;389(1-2):219-27. doi: 10.1007/s11010-013-1943-9. Epub 2013 Dec 31. Mol Cell Biochem. 2014. PMID: 24378994
-
Conductance catheter measurement and effect of different anesthetics in a rat model of postresuscitation myocardial dysfunction.J Am Assoc Lab Anim Sci. 2014 Jul;53(4):392-8. J Am Assoc Lab Anim Sci. 2014. PMID: 25199096 Free PMC article.
-
Towards active tracking of beating heart motion in the presence of arrhythmia for robotic assisted beating heart surgery.PLoS One. 2014 Jul 21;9(7):e102877. doi: 10.1371/journal.pone.0102877. eCollection 2014. PLoS One. 2014. PMID: 25048462 Free PMC article.
-
New parameters for left ventricular function in atrial fibrillation: based on the relationship between RR interval and performance.J Korean Med Sci. 2005 Feb;20(1):20-5. doi: 10.3346/jkms.2005.20.1.20. J Korean Med Sci. 2005. PMID: 15716596 Free PMC article.
References
-
- Brookes CIO, White PA, Staples M, et al. Myocardial contractility is not constant during spontaneous atrial fibrillation in patients. Circulation 1998;98:1762–8. - PubMed
-
- Hardman SM, Noble MIM, Biggs T, et al. Evidence for an influence of mechanical restitution on beat-to-beat variations in haemodynamics during chronic atrial fibrillation in patients. Cardiovasc Res 1998;38:82–90. - PubMed
-
- Hardman SM, Noble MIM, Seed WA. Postextrasystolic potentiation and its contribution to the beat-to-beat variation of the pulse during atrial fibrillation. Circulation 1992;86:1223–32. - PubMed
-
- Hardman SM, Pfeiffer KP, Kenner T, et al. Analysis of left ventricular contractile behaviour during atrial fibrillation. Basic Res Cardiol 1994;89:438–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical