

Interleukin-10 controls the onset of irreversible septic shock
- PMID: 12117955
- PMCID: PMC128185
- DOI: 10.1128/IAI.70.8.4441-4446.2002
Interleukin-10 controls the onset of irreversible septic shock
Abstract
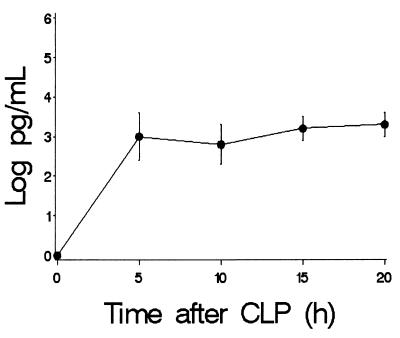
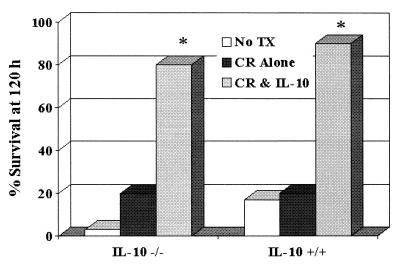
Lethality from sepsis is believed to be mediated by a proinflammatory cytokine cascade, yet blocking the proinflammatory cytokines tumor necrosis factor alpha (TNF-alpha) and interleukin-1 (IL-1) fails to prevent mortality in human disease and a mouse model of sepsis induced by cecal ligation and puncture (CLP). The role of the antiinflammatory cytokine IL-10 in the CLP model of sepsis is unclear, with either protective or harmful effects demonstrated, depending upon the time of intervention. We therefore hypothesize that IL-10 functions as a temporal regulator of the transition from early reversible sepsis to the late phase of irreversible shock. Transition from reversible sepsis to irreversible shock in the CLP model was defined as the time when removal of the necrotic cecum by rescue surgery is no longer effective. We subjected IL-10-deficient (IL-10(-/-)) and wild-type (IL-10(+/+)) mice to CLP and monitored the progression of sepsis, the onset of irreversible shock, and mortality. Onset of lethality in IL-10(-/-) mice occurred significantly earlier than in IL-10(+/+) mice and was associated with 15-fold-higher serum levels of TNF-alpha and IL-6. Consistent with these findings, the efficacy of rescue surgery after lethal CLP is lost 10 h earlier in IL-10(-/-) mice than in IL-10(+/+) mice. Treatment with recombinant human IL-10 5 h after CLP significantly improved survival and lengthened the therapeutic window for rescue surgery in both strains of mice. These results demonstrate that IL-10 controls the onset of irreversible septic shock after CLP.
Figures





Similar articles
-
Interleukin 10 extends the effectiveness of standard therapy during late sepsis with serum interleukin 6 levels predicting outcome.Shock. 2005 Jun;23(6):521-6. Shock. 2005. PMID: 15897804
-
Anti-tumor necrosis factor antibody therapy fails to prevent lethality after cecal ligation and puncture or endotoxemia.J Immunol. 1992 May 1;148(9):2724-30. J Immunol. 1992. PMID: 1315357
-
Interleukin-10 prevents early cytokine release in severe intraabdominal infection and sepsis.J Surg Res. 1997 Jul 1;70(2):107-12. doi: 10.1006/jsre.1997.5071. J Surg Res. 1997. PMID: 9237883
-
Age- and gender-related differences of the immune function in a murine model of hemorrhagic shock: IL-10 restores immunodepression in aged females without reduction of mortality.Langenbecks Arch Surg. 2007 Sep;392(5):629-38. doi: 10.1007/s00423-007-0152-y. Epub 2007 Mar 2. Langenbecks Arch Surg. 2007. PMID: 17334776
-
Pattern of cytokines and pharmacomodulation in sepsis induced by cecal ligation and puncture compared with that induced by endotoxin.Clin Diagn Lab Immunol. 1995 Sep;2(5):549-53. doi: 10.1128/cdli.2.5.549-553.1995. Clin Diagn Lab Immunol. 1995. PMID: 8548533 Free PMC article.
Cited by
-
The effect of conventional and mini-invasive cardiopulmonary bypass on neutrophil activation in patients undergoing coronary artery bypass grafting.Mediators Inflamm. 2012;2012:152895. doi: 10.1155/2012/152895. Epub 2012 Feb 19. Mediators Inflamm. 2012. PMID: 22529517 Free PMC article.
-
PAD4-deficiency does not affect bacteremia in polymicrobial sepsis and ameliorates endotoxemic shock.Blood. 2015 Mar 19;125(12):1948-56. doi: 10.1182/blood-2014-07-587709. Epub 2015 Jan 26. Blood. 2015. PMID: 25624317 Free PMC article.
-
Anti-tumor necrosis factor VNAR single domains reduce lethality and regulate underlying inflammatory response in a murine model of endotoxic shock.BMC Immunol. 2013 Apr 2;14:17. doi: 10.1186/1471-2172-14-17. BMC Immunol. 2013. PMID: 23548047 Free PMC article.
-
Neonatal sepsis and inflammatory mediators.Mediators Inflamm. 2014;2014:269681. doi: 10.1155/2014/269681. Epub 2014 Dec 30. Mediators Inflamm. 2014. PMID: 25614712 Free PMC article. Review.
-
Interleukin-10-1082 promoter polymorphism in association with cytokine production and sepsis susceptibility.Intensive Care Med. 2006 Feb;32(2):260-266. doi: 10.1007/s00134-005-0022-4. Epub 2006 Jan 25. Intensive Care Med. 2006. PMID: 16435103
References
-
- Baker, C. C., I. H. Chaudry, H. O. Gaines, and A. E. Baue. 1983. Evaluations of factors affecting mortality rate after sepsis in a murine cecal ligation and puncture model. Surgery 94:331-335. - PubMed
-
- Balk, R. A. 2000. Severe sepsis and septic shock: definitions, epidemiology, and clinical manifestations. Crit. Care Clin. 16:179-192. - PubMed
-
- Berg, D. J., K. Kuhn, K. Rajewsky, W. Muller, S. Menon, N. Davidson, G. Grunig, and D. Rennick. 1995. Interleukin-10 is a central regulator of the response to LPS in murine models of endotoxic shock and the Shwartzman reaction but not endotoxin tolerance. J. Clin. Investig. 96:2339-2347. - PMC - PubMed
-
- Beutler, B., I. W. Milsark, and A. C. Cerami. 1985. Passive immunization against cachectin/tumor necrosis factor protects mice from lethal effect of endotoxin. Science 229:869-871. - PubMed
-
- Cain, B. S., D. R. Meldrum, A. H. Harken, and R. C. McIntyre. 1998. The physiologic basis for anticytokine clinical trials in the treatment of sepsis. J. Am. Coll. Surg. 186:337-351. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
