

A meta-analysis on the efficacy of preoperative biliary drainage for tumors causing obstructive jaundice
- PMID: 12131081
- PMCID: PMC1422544
- DOI: 10.1097/00000658-200207000-00005
A meta-analysis on the efficacy of preoperative biliary drainage for tumors causing obstructive jaundice
Abstract
Objective: To review the effectiveness of preoperative biliary drainage (PBD) in patients with obstructive jaundice resulting from tumors.
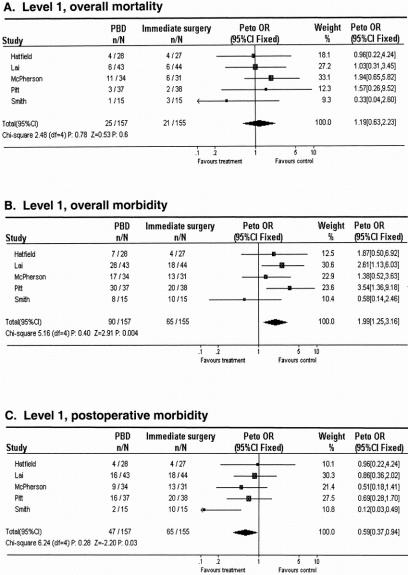
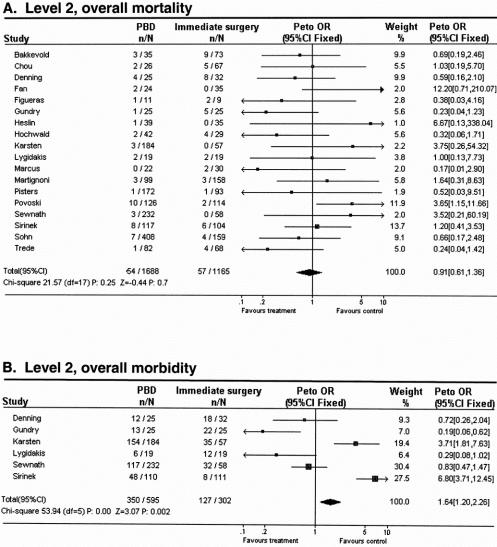
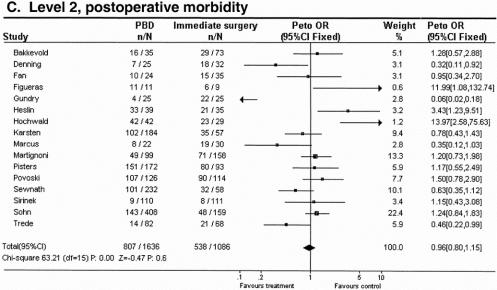
Summary background data: This was a systematic review, including a meta-analysis, of randomized controlled trials and comparative cohort studies conducted worldwide and published between 1966 and September 2001, classified on methodologic strength and subdivided into level 1 (randomized controlled trials) and level 2 (comparative cohort studies).
Methods: Comparison was made of PBD versus no PBD in jaundiced patients undergoing resection of a tumor. Outcome measures were in-hospital death rate, overall complications resulting from the treatment modality (drainage- and surgery-related complications), and hospital stay. Effect sizes were calculated and combined in meta-analyses. Relative differences (%) were calculated to compare effects on outcome measures.
Results: Five randomized controlled studies comprising 302 patients met the inclusion criteria for level 1 studies, and 18 cohort studies comprising 2,853 patients met the criteria for level 2 studies. Meta-analysis of level 1 studies showed no difference in the overall death rate between patients who had PBD and those who had surgery without PBD. The overall complication rate, however, was significantly adversely affected by PBD compared with surgery without PBD. At level 2, there was no difference in the death rate between the two treatment modalities. The overall complication rate, however, was significantly adversely affected by PBD compared with surgery without PBD. If PBD had been without complications, then complications would be in favor of drainage based on level 1 studies, and no difference based on level 2 studies. Further, PBD was not able to reduce the length of postoperative hospital stay compared with surgery without PBD; instead, it prolonged the stay.
Conclusions: This meta-analysis shows that PBD with current standards for patients with obstructive jaundice resulting from tumors carries no benefit and should not be performed routinely. The potential benefit of PBD in terms of postoperative rates of death and complications does not outweigh the disadvantage of the drainage procedure. Only if PBD-related complications could be reduced by 27% and consequently diminish hospital stay could PBD be beneficial. Further randomized controlled trials with improved PBD techniques are necessary.
Figures
Comment in
-
Comment and perspective on Sewnath and colleagues' recent meta-analysis of the efficacy of preoperative biliary drainage for tumors causing obstructive jaundice.Ann Surg. 2003 Apr;237(4):594-5; author reply 595-6. doi: 10.1097/00000658-200304000-00024. Ann Surg. 2003. PMID: 12677158 Free PMC article. No abstract available.
References
-
- Armstrong CP, Dixon JM, Taylor TV, et al. Surgical experience of deeply jaundiced patients with bile duct obstruction. Br J Surg 1984; 71: 234–238. - PubMed
-
- Greig JD, Krukowski ZH, Matheson NA. Surgical morbidity and mortality in one hundred and twenty-nine patients with obstructive jaundice. Br J Surg 1988; 75: 216–219. - PubMed
-
- Blamey SL, Fearon KC, Gilmour WH, et al. Prediction of risk in biliary surgery. Br J Surg 1983; 70: 535–538. - PubMed
-
- Kawarada Y, Higashiguchi T, Yokoi H, et al. Preoperative biliary drainage in obstructive jaundice. Hepato-Gastroenterology 1995; 42: 300–307. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
