

Long-term prognostic significance of extent of rectal cancer response to preoperative radiation and chemotherapy
- PMID: 12131088
- PMCID: PMC1422551
- DOI: 10.1097/00000658-200207000-00012
Long-term prognostic significance of extent of rectal cancer response to preoperative radiation and chemotherapy
Abstract
Objective: To determine whether selected clinicopathologic factors, including the extent of pathologic response to preoperative radiation and chemotherapy (RT +/- chemo), have an impact on long-term recurrence-free survival (RFS) in patients with locally advanced primary rectal cancer after optimal multimodality therapy.
Summary background data: Although complete pathologic response to preoperative RT +/- chemo has been detected in up to 30% of rectal cancers, its significance on long-term outcome has not been widely reported. Previous retrospective studies evaluating clinical outcome in patients with complete or near-complete pathologic response documented good prognosis in this population but were limited by median follow-up in the range of 2 to 3 years.
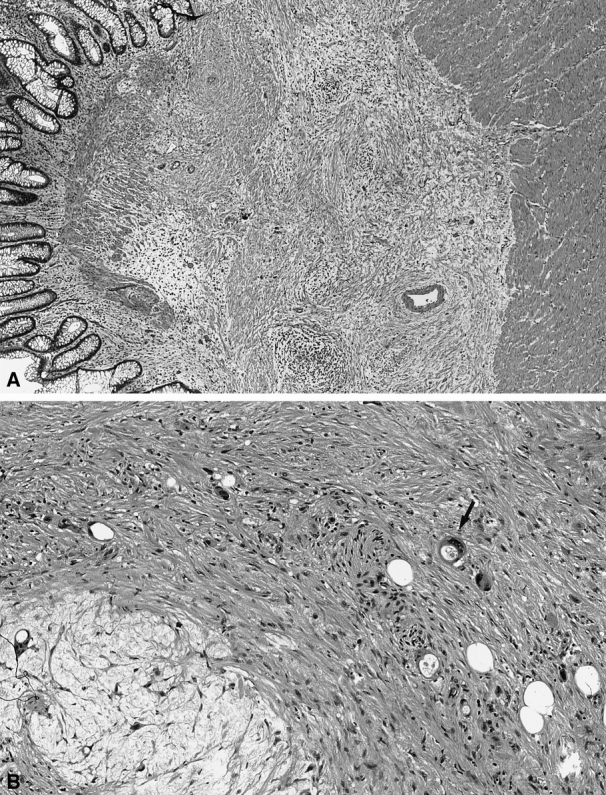
Methods: Sixty-nine patients with locally advanced (T(3-4) and/or N1) primary rectal cancer were prospectively identified. All were treated at one institution with preoperative RT to the pelvis (at least 4,500 cGy). Forty patients received concurrent preoperative 5-fluorouracil-based chemotherapy and 27 received both pre- and postoperative chemotherapy. Patients underwent resection 4 to 7 weeks after completion of RT. TNM stage, angiolymphatic or perineural invasion, and extent of response to preoperative RT +/- chemo were determined by pathologic evaluation. Adverse pathologic features were defined as the presence of angiolymphatic and/or perineural invasion. RFS at 5 years was determined by the Kaplan-Meier method.
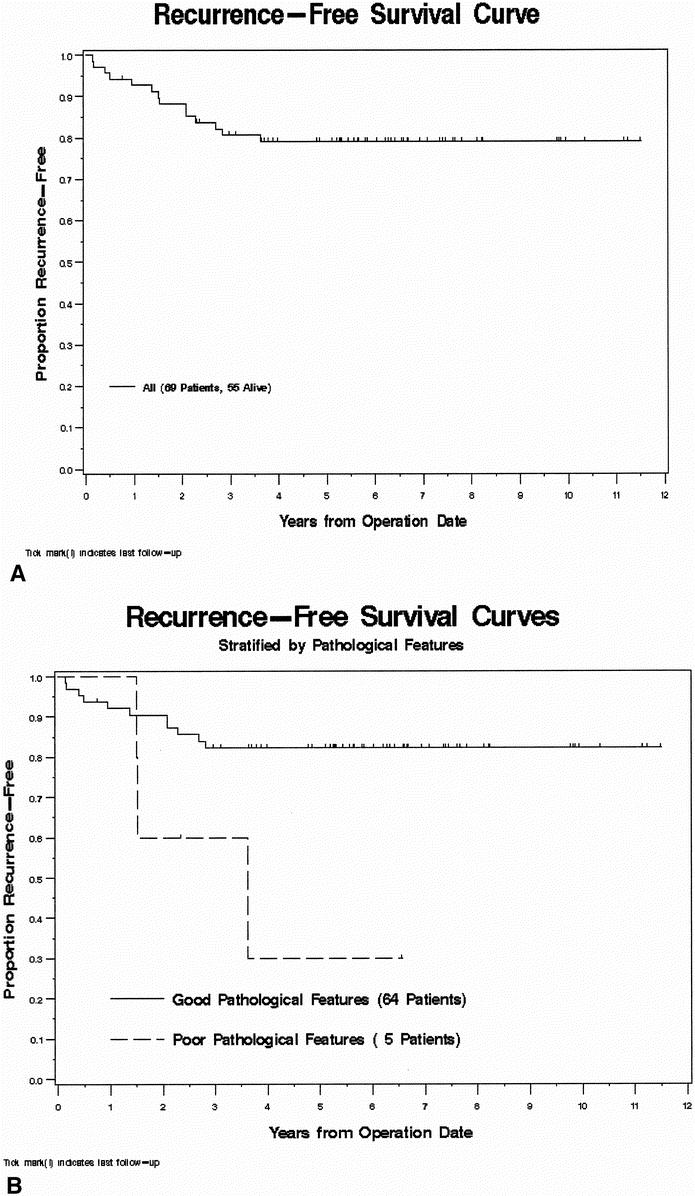
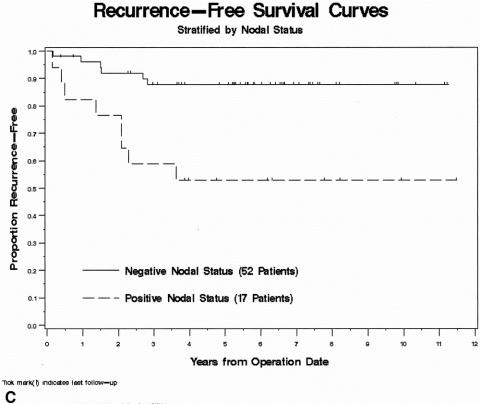
Results: With a median follow-up of 69 months, 5-year RFS was 79%. RFS was significantly worse for patients with aggressive pathologic features and positive nodal status identified in the postirradiated surgical specimen. Risk ratios for RFS were 3.68 for the presence of aggressive pathologic features and 4.64 for node-positive rectal cancers. In patients with greater than 95% rectal cancer response to preoperative RT +/- chemo, only one patient has died as a consequence of cancer, another has died of an unrelated cause, and the remainder were free of disease with a minimum follow-up of 47 months.
Conclusions: These data suggest that a marked response to preoperative RT +/- chemo may be associated with good long-term outcome but was not predictive of RFS. The presence of poor histopathologic features and positive nodal status are the most important prognostic indicators after neoadjuvant therapy.
Figures
References
-
- NIH Consensus Conference. Adjuvant therapy for patients with colon and rectal cancer. JAMA 1990; 264: 1444–1450. - PubMed
-
- Minsky BD, Cohen AM, Kemeny N, et al. Combined modality therapy of rectal cancer: decreased acute toxicity with the preoperative approach. J Clin Oncol 1992; 10: 1218–1224. - PubMed
-
- Minsky BD, Coia L, Haller DG, et al. Radiation therapy for rectosigmoid and rectal cancer: results of the 1992–1994 Patterns of Care process survey. J Clin Oncol 1998; 16: 2542–2547. - PubMed
-
- Valentini V, Coco C, Cellini N, et al. Preoperative chemoradiation for extraperitoneal T3 rectal cancer: acute toxicity, tumor response, and sphincter preservation. Int J Radiat Oncol Biol Phys 1998; 40: 1067–1075. - PubMed
-
- Pucciarelli S, Friso ML, Toppan P, et al. Preoperative combined radiotherapy and chemotherapy for middle and lower rectal cancer: preliminary results. Ann Surg Oncol 2000; 7: 38–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
