

Pneumococcal disease in HIV-infected Malawian adults: acute mortality and long-term survival
- PMID: 12131218
- PMCID: PMC5068550
- DOI: 10.1097/00002030-200207050-00013
Pneumococcal disease in HIV-infected Malawian adults: acute mortality and long-term survival
Abstract
Objective: HIV-infected patients in Africa are vulnerable to severe recurrent infection with Streptococcus pneumoniae, but no effective preventive strategy has been developed. We set out to determine which factors influence in-hospital mortality and long-term survival of Malawians with invasive pneumococcal disease.
Design, setting and patients: Acute clinical features, inpatient mortality and long-term survival were described among consecutively admitted hospital patients with S. pneumoniae in the blood or cerebrospinal fluid. Factors associated with inpatient mortality were determined, and patients surviving to discharge were followed to determine their long-term outcome.
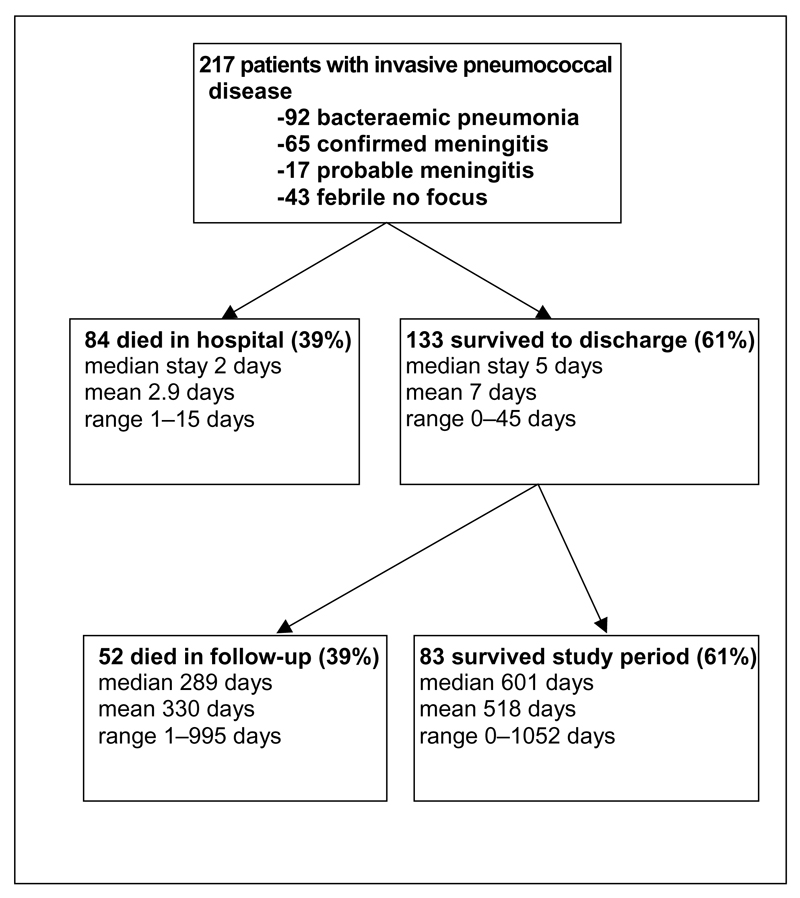
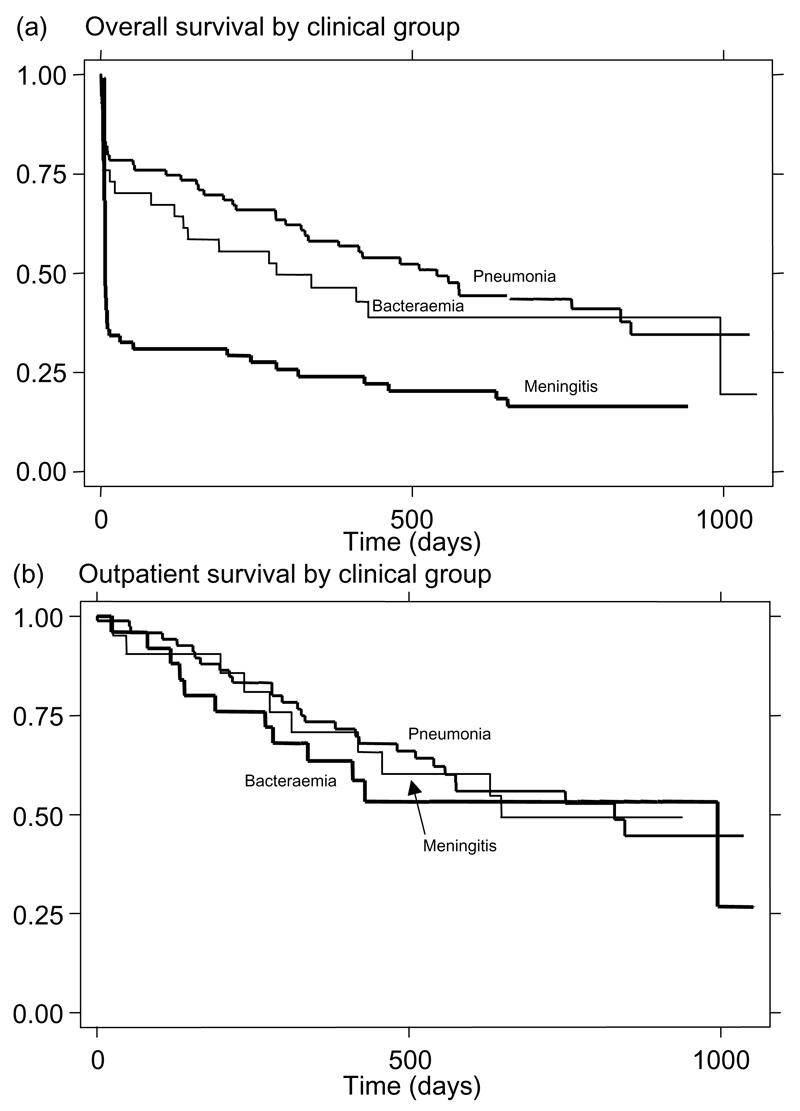
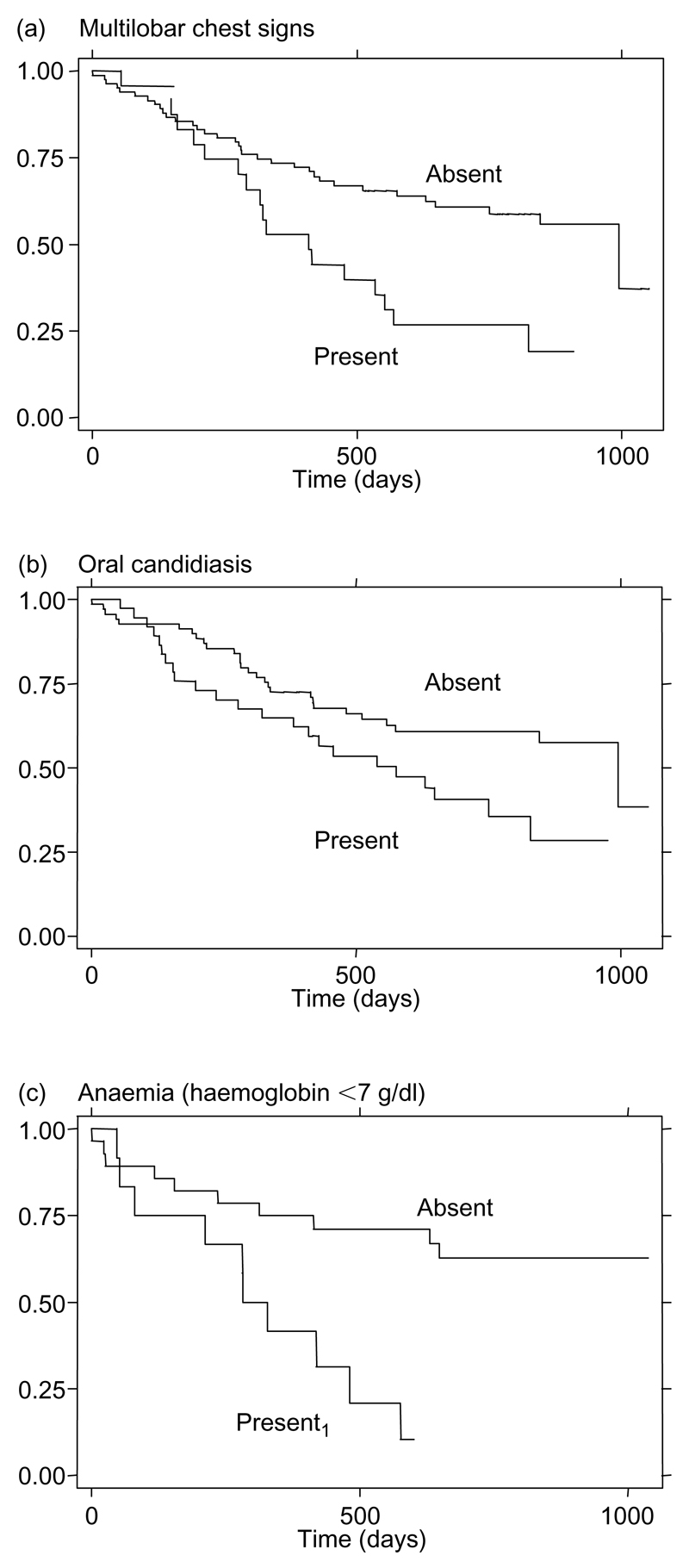
Results: A total of 217 patients with pneumococcal disease were studied over an 18-month period. Among these, 158 out of 167 consenting to testing (95%) were HIV positive. Inpatient mortality was 65% for pneumococcal meningitis (n = 64), 20% for pneumococcaemic pneumonia (n = 92), 26% for patients with pneumococcaemia without localizing signs (n = 43), and 76% in patients with probable meningitis (n = 17). Lowered consciousness level, hypotension, and age exceeding 55 years at presentation were associated with inpatient death, but not long-term outcome in survivors. Hospital survivors were followed for a median of 414 days; 39% died in the community during the study period. Outpatient death was associated with multilobar chest signs, oral candidiasis, and severe anaemia as an inpatient.
Conclusion: Most patients with pneumococcal disease in Malawi have HIV co-infection. They have severe disease with a high mortality rate. At discharge, all HIV-infected adults have a poor prognosis but patients with multilobar chest signs or anaemia are at particular risk.
Figures
References
-
- Gilks CF, Brindle RJ, Otieno LS, et al. Life-threatening bacteraemia in HIV-1 seropositive adults admitted to hospital in Nairobi, Kenya. Lancet. 1990;336:545–549. - PubMed
-
- Gilks CF, Ojoo SA, Ojoo JC, et al. Invasive pneumococcal disease in a cohort of predominantly HIV-1 infected female sex-workers in Nairobi, Kenya. Lancet. 1996;347:718–723. - PubMed
-
- Redd SC, Rutherford GW, Sande MA, et al. The role of human immunodeficiency virus in pneumococcal bacteraemia in San Francisco residents. J Infect Dis. 1990;162:1012–1017. - PubMed
-
- Hibbs JR, Douglas JMJ, Judson FN, et al. Prevalence of human immunodeficiency virus infection, mortality rate, and serogroup distribution among patients with pneumococcal bacteremia at Denver General Hospital, 1984–1994. Clin Infect Dis. 1997;25:195–199. - PubMed
-
- Frankel RE, Virata M, Hardalo C, Altice FL, Friedland G. Invasive pneumococcal disease: clinical features, serotypes, and antimicrobial resistance patterns in cases involving patients with and without human immunodeficiency virus infection. Clin Infect Dis. 1996;23:577–584. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
