

The relationship of post-acute home care use to Medicaid utilization and expenditures
- PMID: 12132601
- PMCID: PMC1434657
- DOI: 10.1111/1475-6773.00044
The relationship of post-acute home care use to Medicaid utilization and expenditures
Abstract
Research objectives: To describe the use of post-acute home care (PAHC) and total Medicaid expenditures among hospitalized nonelderly adult Medicaid eligibles and to test whether health services utilization rates or total Medicaid expenditures were lower among Medicaid eligibles who used PAHC compared to those who did not.
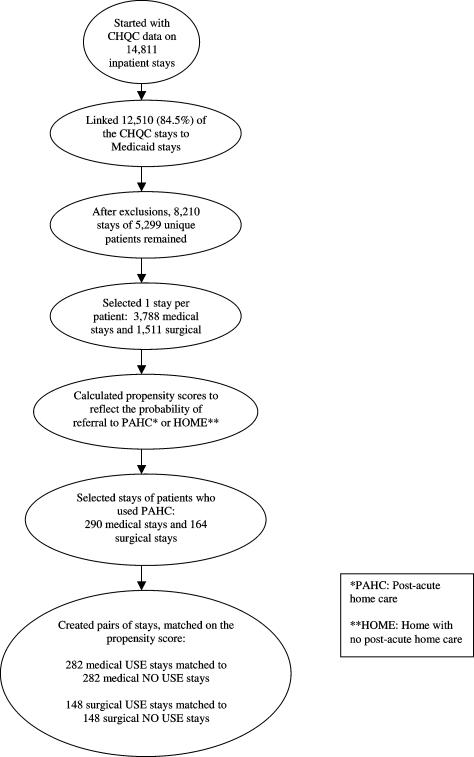
Study population: 5,299 Medicaid patients aged 18-64 discharged in 1992-1996 from 29 hospitals in the Cleveland Health Quality Choice (CHQC) project.
Data sources: Linked Ohio Medicaid claims and CHQC medical record abstract data.
Data extraction: One stay per patient was randomly selected.
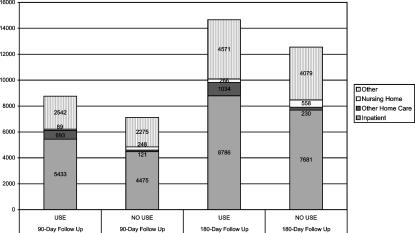
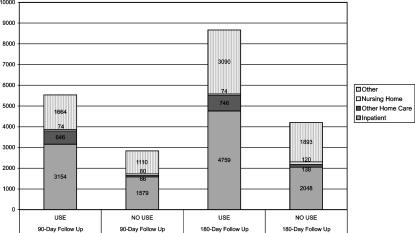
Design: Observational study. To control for treatment selection bias, we developed a model predicting the probability (propensity) a patient would be referred to PAHC, as a proxy for the patient's need for PAHC. We matched 430 patients who used Medicaid-covered PAHC ("USE") to patients who did not ("NO USE") by their propensity scores. Study outcomes were inpatient re-admission rates and days of stay (DOS), nursing home admission rates and DOS, and mean total Medicaid expenditures 90 and 180 days after discharge.
Principal findings: Of 3,788 medical patients, 12.1 percent were referred to PAHC; 64 percent of those referred used PAHC. Of 1,511 surgical patients, 10.9 percent were referred; 99 percent of those referred used PAHC. In 430 pairs of patients matched by propensity score, mean total Medicaid expenditures within 90 days after discharge were $7,649 in the USE group and $5,761 in the NO USE group. Total Medicaid expenditures were significantly higher in the USE group compared to the NO USE group for medical patients after 180 days (p < .05) and surgical patients after 90 and 180 days (p < .001). There were no significant differences for any other outcome. Sensitivity analysis indicates the results may be influenced by unmeasured variables, most likely functional status and/or care-giver support.
Conclusions: Thirty-six percent of the medical patients referred to PAHC did not receive Medicaid-covered services. This suggests potential underuse among medical patients. The high post-discharge expenditures suggest opportunities for reducing costs through coordinating utilization or diverting it to lower-cost settings. Controlling for patients' need for services, PAHC utilization was not associated with lower utilization rates or lower total Medicaid expenditures. Medicaid programs are advised to proceed cautiously before expanding PAHC utilization and to monitor its use carefully. Further study, incorporating non-economic outcomes and additional factors influencing PAHC use, is warranted.
Figures
Similar articles
-
Comparison of resource utilization for Medicaid dementia patients using nursing homes versus home and community based waivers for long-term care.Med Care. 2008 Apr;46(4):449-53. doi: 10.1097/MLR.0b013e3181621eae. Med Care. 2008. PMID: 18362827
-
How does Cash and Counseling affect costs?Health Serv Res. 2007 Feb;42(1 Pt 2):488-509. doi: 10.1111/j.1475-6773.2006.00680.x. Health Serv Res. 2007. PMID: 17244294 Free PMC article. Clinical Trial.
-
Cost Analysis of Physician Assistant Home Visit Program to Reduce Readmissions After Cardiac Surgery.Ann Thorac Surg. 2016 Sep;102(3):696-702. doi: 10.1016/j.athoracsur.2016.03.077. Epub 2016 May 25. Ann Thorac Surg. 2016. PMID: 27234575
-
Home-Based Primary and Palliative Care in the Medicaid Program: Systematic Review of the Literature.J Am Geriatr Soc. 2021 Jan;69(1):245-254. doi: 10.1111/jgs.16837. Epub 2020 Sep 21. J Am Geriatr Soc. 2021. PMID: 32959375 Free PMC article.
-
What Happens After a Patient Safety Event? Medical Expenditures and Outcomes in Medicare.In: Henriksen K, Battles JB, Marks ES, Lewin DI, editors. Advances in Patient Safety: From Research to Implementation (Volume 1: Research Findings). Rockville (MD): Agency for Healthcare Research and Quality (US); 2005 Feb. In: Henriksen K, Battles JB, Marks ES, Lewin DI, editors. Advances in Patient Safety: From Research to Implementation (Volume 1: Research Findings). Rockville (MD): Agency for Healthcare Research and Quality (US); 2005 Feb. PMID: 21249795 Free Books & Documents. Review.
Cited by
-
The Relationship between Substance Abuse Performance Measures and Mutual Help Group Participation after Treatment.Alcohol Treat Q. 2012;30(2):190-210. doi: 10.1080/07347324.2012.663305. Epub 2012 Apr 13. Alcohol Treat Q. 2012. PMID: 22879689 Free PMC article.
-
Home health care: healing where the heart is.Mo Med. 2012 Nov-Dec;109(6):439-42. Mo Med. 2012. PMID: 23362645 Free PMC article. No abstract available.
-
Choosing the Best and Scrambling for the Rest: Hospital-Nursing Home Relationships and Admissions to Post-Acute Care.J Appl Gerontol. 2019 Apr;38(4):479-498. doi: 10.1177/0733464817752084. Epub 2018 Jan 7. J Appl Gerontol. 2019. PMID: 29307258 Free PMC article.
References
-
- Arnold S, Gage B, Harris J. Interim Analysis of Payment Reform for Home Health Services. Washington DC: Prospective Payment Commission; 1994.
-
- Ash AS, Shwartz M, Iezzoni LI. Risk Adjustment for Measuring Healthcare Outcomes. Chicago: Health Administration Press; 1997. “Evaluating the Performance of Risk-Adjustment Methods: Dichotomous Measures”; pp. 427–71.
-
- Blewett LA, Kane RL, Finch M. “Hospital Ownership of Post-Acute Care: Does It Increase Access to Post-Acute Care Services?”. Inquiry. 1995–1996;32(4):457–67. - PubMed
-
- Bureau of Labor Statistics. In Statistical Abstract of the United States: 1998. Washington DC: U.S. Bureau of the Census; 1998. “Consumer Price Indexes of Medical Care Prices: 1980–1998”; p. 124.
-
- Chappell NL. “Home Care Research: What Does It Tell Us?”. The Gerontologist. 1994;34(1):116–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
