

Designing and evaluating interventions to eliminate racial and ethnic disparities in health care
- PMID: 12133164
- PMCID: PMC1495065
- DOI: 10.1046/j.1525-1497.2002.10633.x
Designing and evaluating interventions to eliminate racial and ethnic disparities in health care
Abstract
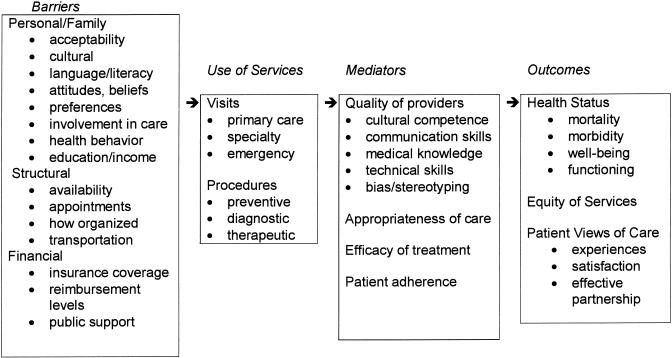
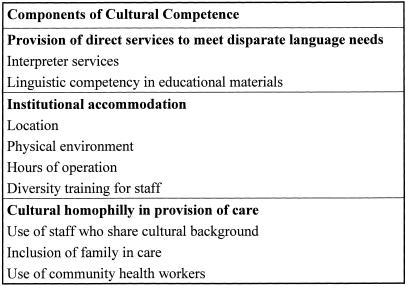
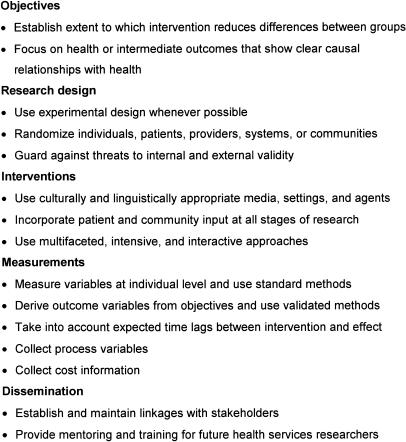
A large number of factors contribute to racial and ethnic disparities in health status. Health care professionals, researchers, and policymakers have believed for some time that access to care is the centerpiece in the elimination of these health disparities. The Institute of Medicine's (IOM) model of access to health services includes personal, financial, and structural barriers, health service utilization, and mediators of care. This model can be used to describe the interactions among these factors and their impact on health outcomes and equity of services among racial and ethnic groups. We present a modified version of the IOM model that incorporates the features of other access models and highlights barriers and mediators that are relevant for interventions designed to eliminate disparities in U.S. health care. We also suggest that interventions to eliminate disparities and achieve equity in health care services be considered within the broader context of improving quality of care. Some health service intervention studies have shown improvements in the health of disadvantaged groups. If properly designed and implemented, these interventions could be used to reduce health disparities. Successful features of interventions include the use of multifaceted, intense approaches, culturally and linguistically appropriate methods, improved access to care, tailoring, the establishment of partnerships with stakeholders, and community involvement. However, in order to be effective in reducing disparities in health care and health status, important limitations of previous studies need to be addressed, including the lack of control groups, nonrandom assignment of subjects to experimental interventions, and use of health outcome measures that are not validated. Interventions might be improved by targeting high-risk populations, focusing on the most important contributing factors, including measures of appropriateness and quality of care and health outcomes, and prioritizing dissemination efforts.
Figures
References
-
- Andrulis DP. Access to care is the centerpiece in the elimination of socioeconomic disparities in health. Ann Intern Med. 1998;129:412–6. - PubMed
-
- Weissman JS, Stern R, Fielding SL, Epstein AM. Delayed access to health care: risk factors, reasons, and consequences. Ann Intern Med. 1991;114:325–31. - PubMed
-
- Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19:127–40. - PubMed
-
- Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19–22 June, 1946; signed on 22 July 1946 by the representatives of 61 states (Official Records of the World Health Organization, No. 2, pg 100) and entered into force on 7 April 1948.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources