

Review
doi: 10.1186/cc1492.
Epub 2002 Apr 25.
Equipment review: new techniques for cardiac output measurement--oesophageal Doppler, Fick principle using carbon dioxide, and pulse contour analysis
Affiliations
- PMID: 12133181
- PMCID: PMC137448
- DOI: 10.1186/cc1492
Item in Clipboard
Review
Equipment review: new techniques for cardiac output measurement--oesophageal Doppler, Fick principle using carbon dioxide, and pulse contour analysis
Crit Care.
2002 Jun.
Abstract
Measuring cardiac output is of paramount importance in the management of critically ill patients in the intensive care unit and of 'high risk' surgical patients in the operating room. Alternatives to thermodilution are now available and are gaining acceptance among practitioners who have been trained almost exclusively in the use of the pulmonary artery catheter. The present review focuses on the principles, advantages and limitations of oesophageal Doppler, Fick principle applied to carbon dioxide, and pulse contour analysis. No single method stands out or renders the others obsolete. By making cardiac output easily measurable, however, these techniques should all contribute to improvement in haemodynamic management.
Figures
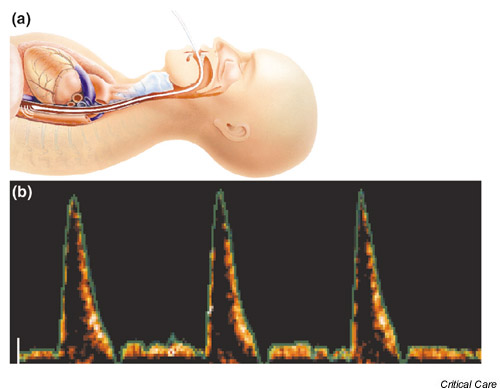
Oesophageal Doppler. (a) Schematic representation of oesophageal Doppler probe in a patient, demonstrating the close relation between oesophagus and descending thoracic aorta. (b) Characteristic velocity waveform obtained in the descending aorta. The spectral representation shows that most red blood cells (orange-white color) are moving at the maximum velocity (close to the green envelope) during systole, and that diastolic flow is minimal.
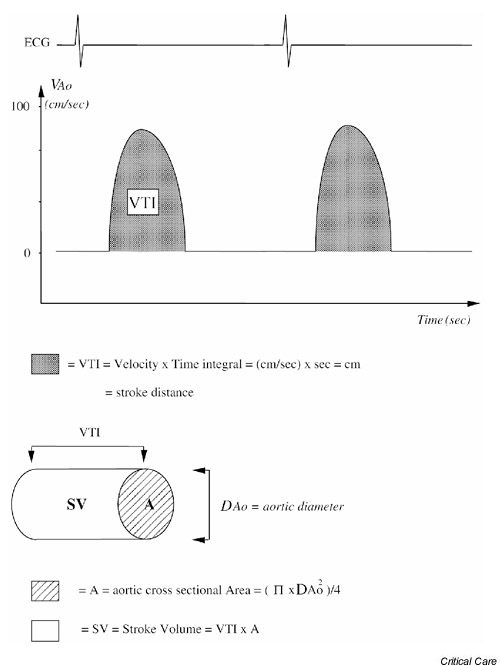
Principle of stroke volume calculation from aortic velocity (VAo) measurements. The area under the maximum aortic velocity envelope (VTI) represents the stroke distance. Assuming that all red blood cells are moving at maximum velocity and that aortic cross-sectional area is constant during systole, stroke volume is obtained by multiplying stroke distance by aortic cross-sectional area.
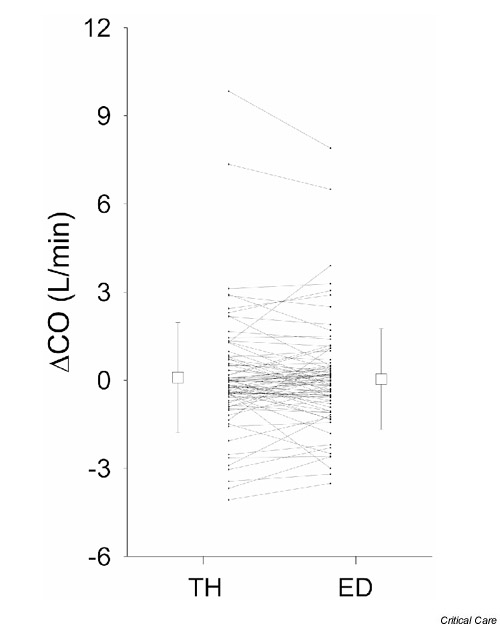
Eighty-eight paired measurements of cardiac output (CO) variations between two time-points obtained simultaneously using thermodilution (TH) with a pulmonary artery catheter and oesophageal Doppler (ED). Ideal agreement is represented by a horizontal line. Contradictory information with the two techniques was observed in only three cases [10]. The open boxes and vertical bars indicate mean and standard deviation, respectively.
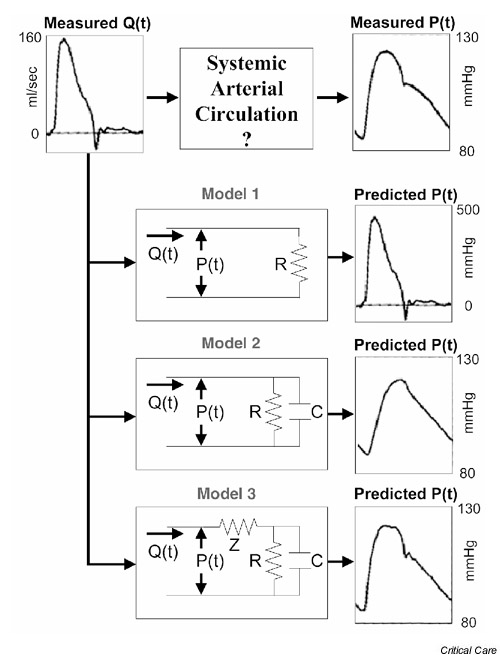
Illustration of the importance of various arterial mechanical properties in generating the aortic pressure waveform. With the measured instantaneous flow [Q(t)] as an input, a single resistance (R) model of the circulation (model 1) would generate a pressure waveform [P(t)] with morphology identical to that of the flow waveform, differing only in magnitude by a factor of R. When arterial compliance, represented by a capacitance element (C), is incorporated (model 2), the predicted pressure waveform begins to exhibit many of the morphological characteristics of its measured counterpart. If a third element representing characteristic impedance (Z) is introduced (model 3), the morphologies of the predicted and measured pressure waveforms become very similar [23].
Similar articles
-
Noninvasive techniques for measurements of cardiac output.Curr Opin Crit Care. 2005 Oct;11(5):424-9. doi: 10.1097/01.ccx.0000176698.51456.5a. Curr Opin Crit Care. 2005. PMID: 16175028 Review.
-
Accuracy of cardiac output measurements with pulse contour analysis (PulseCO) and Doppler echocardiography during off-pump coronary artery bypass grafting.Eur J Anaesthesiol. 2008 Mar;25(3):243-8. doi: 10.1017/S0265021507002979. Epub 2007 Nov 9. Eur J Anaesthesiol. 2008. PMID: 17996125
-
Comparison of esophageal Doppler, pulse contour analysis, and real-time pulmonary artery thermodilution for the continuous measurement of cardiac output.J Cardiothorac Vasc Anesth. 2004 Apr;18(2):185-9. doi: 10.1053/j.jvca.2004.01.025. J Cardiothorac Vasc Anesth. 2004. PMID: 15073709 Clinical Trial.
-
Cardiac output monitoring.Ann Card Anaesth. 2008 Jan-Jun;11(1):56-68. doi: 10.4103/0971-9784.38455. Ann Card Anaesth. 2008. PMID: 18182765 Review.
-
Oxygen Fick and modified carbon dioxide Fick cardiac outputs.Crit Care Med. 1994 Jan;22(1):86-95. doi: 10.1097/00003246-199401000-00018. Crit Care Med. 1994. PMID: 8124981
Cited by
-
Validation of a continuous, arterial pressure-based cardiac output measurement: a multicenter, prospective clinical trial.Crit Care. 2007;11(5):R105. doi: 10.1186/cc6125. Crit Care. 2007. PMID: 17880692 Free PMC article. Clinical Trial.
-
Clinical review: New technologies -- venturing out of the intensive care unit.Crit Care. 2005 Jun;9(3):296-302. doi: 10.1186/cc2982. Epub 2004 Nov 2. Crit Care. 2005. PMID: 15987384 Free PMC article. Review.
-
Estimation of cardiac output and pulmonary vascular resistance by contrast echocardiography transit time measurement: a prospective pilot study.Cardiovasc Ultrasound. 2014 Oct 31;12:44. doi: 10.1186/1476-7120-12-44. Cardiovasc Ultrasound. 2014. PMID: 25361851 Free PMC article.
-
Estimating cardiac output based on gas exchange during veno-arterial extracorporeal membrane oxygenation in a simulation study using paediatric oxygenators.Sci Rep. 2021 Jun 1;11(1):11528. doi: 10.1038/s41598-021-90747-w. Sci Rep. 2021. PMID: 34075067 Free PMC article.
-
A novel approach to measure cardiac output noninvasively: a comparison with the thermodilution method on critical care patients.J Clin Monit Comput. 2004 Jun;18(3):189-97. doi: 10.1023/b:jocm.0000042917.59182.c5. J Clin Monit Comput. 2004. PMID: 15562985
References
-
- Huntsman LL, Stewart DK, Barnes SR, Franklin SB, Colocousis JS, Hessel EA. Noninvasive Doppler determination of cardiac output in man: clinical validation. Circulation. 1983;67:593–602. - PubMed
-
- Mark JB, Steinbrook RA, Gugino LD, Maddi R, Hartwell B, Shemin R, DiSesa V, Rida WN. Continuous noninvasive monitoring of cardiac output with esophageal Doppler ultrasound during cardiac surgery. Anesth Analg. 1986;65:1013–1020. - PubMed
-
- Perrino AC, Fleming J, LaMantia KR. Transesophageal Doppler cardiac output monitoring: performance during aortic reconstructive surgery. Anesth Analg. 1991;73:705–710. - PubMed
-
- Cariou A, Monchi M, Joly LM, Bellenfant F, Claessens YE, Thebert D, Brunet F, Dhainaut JF. Noninvasive cardiac output monitoring by aortic blood flow determination: evaluation of the Sometec Dynemo-3000 system. Crit Care Med. 1998;26:2066–2072. - PubMed
-
- Singer M, Clarke J, Bennett ED. Continuous hemodynamic monitoring by esophageal Doppler. Crit Care Med. 1989;17:447–452. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
