

Design of the Monitored Occlusion Treatment of Amblyopia Study (MOTAS)
- PMID: 12140215
- PMCID: PMC1771248
- DOI: 10.1136/bjo.86.8.915
Design of the Monitored Occlusion Treatment of Amblyopia Study (MOTAS)
Abstract
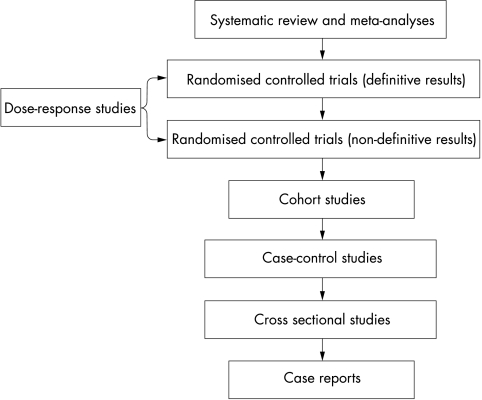
Background/aims: The effectiveness of occlusion therapy for the treatment of amblyopia is a research priority. The authors describe the design of the Monitored Occlusion Treatment for Amblyopia Study (MOTAS) and its methodology. MOTAS will determine the dose-response relation for occlusion therapy as a function of age and category of amblyopia.
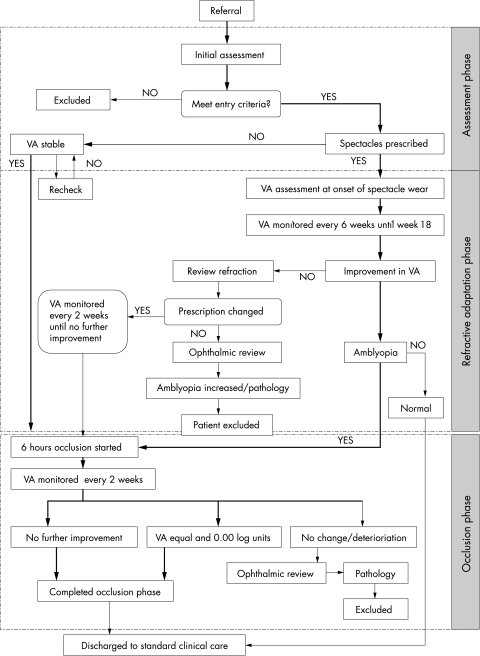
Methods: Subjects progress through up to three study phases: (1) Assessment and baseline phase: On confirmation of eligibility, and after parental consent, baseline visual functions are determined, and spectacles prescribed as necessary; (2) Refractive adaptation phase: Subjects wear spectacles full time and return to clinic at 6 weekly intervals until 18 weeks, by which time all improvement due to refractive correction is complete; (3) Occlusion phase: All subjects are prescribed 6 hours of occlusion per day. Daily occlusion is objectively monitored using an occlusion dose monitor (ODM).
Outcome variables: visual acuity (logMAR charts), log contrast sensitivity (Pelli-Robson chart), and stereoacuity (Frisby) are assessed at 2 weekly intervals until gains in visual acuity cease to be statistically verifiable.
Conclusion: Four methodological issues have been addressed; firstly, baseline stability of visual function; secondly, differentiation of refractive adaptation from occlusion; thirdly, objective measurement of occlusion dose and concordance; fourthly, use of validated outcome measures.
Figures
References
-
- Attebo K, Mitchell P, Cumming R, et al. Prevalence and causes of amblyopia in an adult population. Ophthalmology 1998;105:154–9. - PubMed
-
- Cuiffreda K, Levi D, Selenow A. Amblyopia: basic and clinical aspects. Oxford: Butterworth-Heinemann, 1991.
-
- Hiscox FN, Strong N, Minshull C, et al. Occlusion for amblyopia: a comprehensive survey of outcome. Eye 1992;6:300–4. - PubMed
-
- Snowden S, Stewart-Brown S. Pre-school vision screening: results of a systematic review. CRD Report 9. April 1997.
-
- Watson PG, Sanac AS, Pickering MS. A comparison of various methods of treatment of amblyopia: a block study. Trans Ophthalmol Soc UK 1985;104:319–28. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical