

A chronotherapeutic approach to effective blood pressure management
- PMID: 12147924
- PMCID: PMC8101822
- DOI: 10.1111/j.1524-6175.2002.01035.x
A chronotherapeutic approach to effective blood pressure management
Abstract
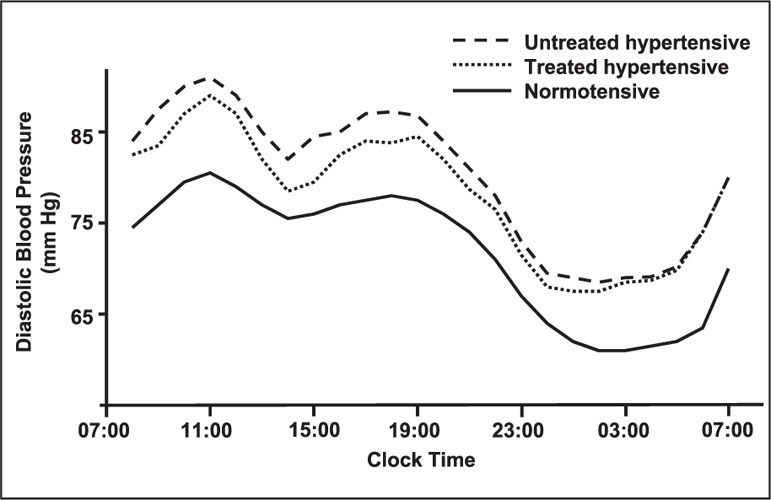
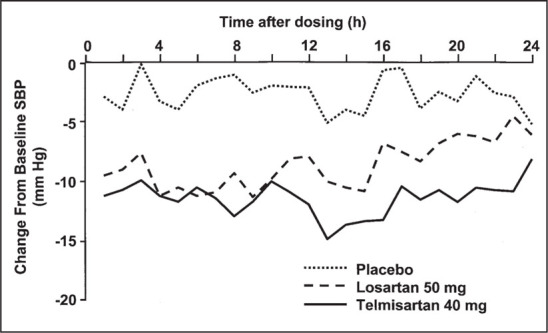
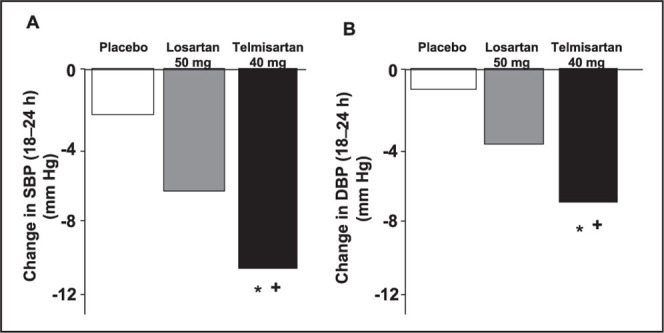
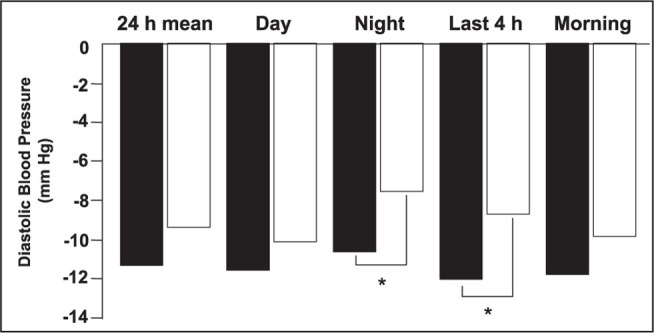
The major randomized trials in hypertension have unequivocally demonstrated the benefits of treatment. None of these trials have sought to address the issue of the potential superiority of 24-hour blood pressure control. However, there is a volume of epidemiologic evidence to suggest that prevention of target organ damage requires the sustained reduction of blood pressure throughout the full 24-hour period between doses. Historically, some antihypertensive drugs have been approved for use at high doses to achieve apparent blood pressure control at the end of the once-daily dosing interval. This approach is flawed; attention is focused on this single time point at the end of the dosing interval, without due regard to the antihypertensive response during the rest of the dosing interval. Subsequently, guidelines formulated by the US Food and Drug Administration suggest that all antihypertensive drugs should consistently achieve a trough:peak ratio decline in blood pressure of at least 50%. Evidence suggests that antihypertensive drugs, such as calcium antagonists and angiotensin II receptor blockers, differ in their ability to provide 24-hour blood pressure control. For example, unlike some other angiotensin II receptor blockers, telmisartan provides consistent reduction of blood pressure during the 24-hour period.
Copyright 2002 Le Jacq Communications, Inc.
Figures
References
-
- Joint National Committee . The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med. 1997;157:2413–2446. - PubMed
-
- Mancia G, Sega R, Milesi C, et al. Blood‐pressure control in the hypertensive population. Lancet. 1997;349:454–457. - PubMed
-
- Neaton JD, Kuller L, Stamler J, et al. Impact of systolic and diastolic blood pressure on cardiovascular mortality. In: Laragh JH, Brenner BM, eds. Hypertension: Pathology, Diagnosis, and Management. 2nd ed. New York, NY:Raven Press; 1995:127–144.
-
- MacMahon S, Peto R, Cutler J, et al. Blood pressure, stroke, and coronary heart disease. Lancet. 1990;335:765–774. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
