

Duct-to-duct biliary reconstruction in living donor liver transplantation utilizing right lobe graft
- PMID: 12170029
- PMCID: PMC1422570
- DOI: 10.1097/00000658-200208000-00012
Duct-to-duct biliary reconstruction in living donor liver transplantation utilizing right lobe graft
Abstract
Objective: To assess the feasibility and safety of duct-to-duct biliary anastomosis for living donor liver transplantation (LDLT) utilizing the right lobe.
Summary background data: Biliary tract complications remain one of the most serious problems after liver transplantation. Roux-en-Y hepaticojejunostomy has been a standard procedure for biliary reconstruction in LDLT with a partial hepatic graft. However, end-to-end choledochocholedochostomy is the technique of choice for biliary reconstruction and yields a more physiologic bilioenteric continuity than can be achieved with Roux-en-Y hepaticojejunostomy. The authors performed right lobe LDLT with end-to-end duct-to-duct biliary anastomosis, and this study assessed retrospectively the relation between the manner of reconstruction and complications.
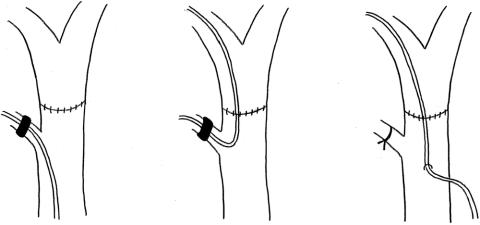
Methods: Between July 1999 and December 2000, 51 patients (11-67 years of age) underwent 52 right lobe LDLTs with duct-to-duct biliary reconstruction and remained alive more than 1 month after their transplantation. Interrupted biliary anastomosis was performed for 24 transplants and the continuous procedure was used for 28. A biliary tube was inserted downward into the common bile ducts through the recipient's cystic duct in 16 transplants (cystic drainage), or a biliary stent tube was pushed upward into the anastomosis through the cystic duct in four transplants (cystic stent), or upward into the anastomosis through the wall of the common bile duct in 31 transplants (external stent).
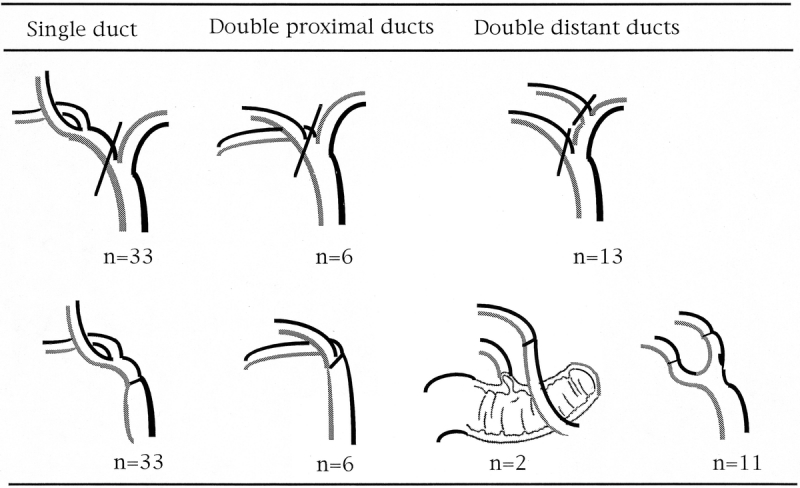
Results: Biliary anastomotic procedures consisted of 34 single end-to-end anastomoses, 11 double end-to-end anastomoses, and 7 single anastomoses for double hepatic ducts. Overall, 5 patients developed leakage (9.6%) and 12 patients suffered stricture (23.0%). For biliary anastomosis with interrupted suture, the incidence of stricture was significantly higher in the cystic drainage group (53.3%, 8/15) than in the stent group consisting of cystic stent and external stent (0%, 0/8). While the respective incidences of leakage and stricture were 20% and 53.3% for intermittent suture with a cystic drainage tube (n = 15), they were 7.7% and 15.4% for a continuous suture with an external stent (n = 26). There was a significant difference in the incidence of stricture.
Conclusions: Duct-to-duct reconstruction with continuous suture combined with an external stent represents a useful technique for LDLT utilizing the right lobe, but biliary complications remain significant.
Figures
References
-
- Egawa H, Uemoto S, Inomata Y, et al. Biliary complications in pediatric living related liver transplantation. Surgery 1998; 124: 901–910. - PubMed
-
- Lopez RR, Benner KG, Ivancev K, et al. Management of biliary complications after liver transplantation. Am J Surg 1992; 163: 519–524. - PubMed
-
- Sawyer RG, Punch JD. Incidence and management of biliary complications after 291 liver transplants following the introduction of transcystic stenting. Transplantation 1998; 66: 1201–1207. - PubMed
-
- Belli L, De Carlis L, Del Favero E, et al. Biliary complications in orthotopic liver transplantation: experience with a modified technique of duct-to-duct reconstruction. Transplant Int 1991; 4: 161–165. - PubMed
-
- Anselmi M, Sherlock D, Buist L, et al. Gallbladder conduit vs end-to-end anastomosis of the common bile duct in orthotopic liver transplantation. Transplant Proc 1990; 22: 2295–2296. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
