

New insights into the mechanism of neurally mediated syncope
- PMID: 12181208
- PMCID: PMC1767328
- DOI: 10.1136/heart.88.3.217
New insights into the mechanism of neurally mediated syncope
Abstract
Objective: To determine the role of the cerebral cortex in neurally mediated syncope, the electroencephalograms (EEG) of patients recorded during head up tilt table test were analysed.
Design: Retrospective study.
Setting: University hospital.
Patients: 18 patients with syncope or near syncope underwent head up tilt table test with simultaneous ECG and EEG monitoring.
Methods: Standard 70 degrees tilt table test was done with simultaneous ECG and EEG monitoring. EEG waveforms were analysed by both visual inspection and spectral analysis.
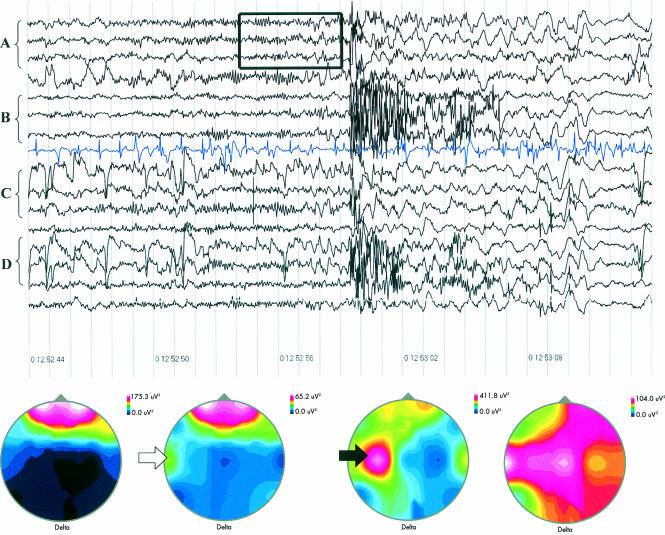
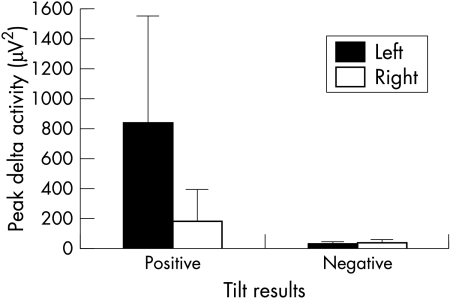
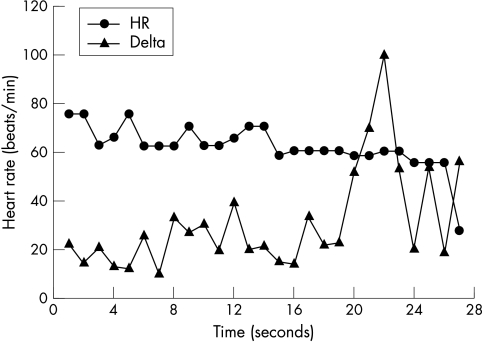
Results: 6 of 18 patients (33%) had a positive tilt table test. Before syncope slow waves increased in patients with a positive test. In addition, five of six tilt positive patients (83%) had slow wave activity that lateralised to the left side of the brain (mean (SD) 822 (724) v 172 (215) micro V(2), p < 0.05), while none of the tilt negative patients exhibited lateralisation (24 (15) v 26 (19) micro V(2), NS). Spectral analysis showed that the lateralisation occurred in the delta frequency. The lateralisation preceded the event by 5-56 seconds (18 (21) seconds).
Conclusions: EEG activity lateralises to the left hemisphere of the brain before syncope. The lateralisation precedes syncope and is associated with the onset of bradycardia, hypotension, and clinical symptoms. These findings suggest that the central nervous system may have a role in neurally mediated syncope.
Figures

Comment in
-
Syncope: what is the trigger?Heart. 2003 Feb;89(2):123-4. doi: 10.1136/heart.89.2.123. Heart. 2003. PMID: 12527651 Free PMC article.
Similar articles
-
The clinical utility of qualitative electroencephalography during tilt table testing - A retrospective study.Clin Neurophysiol. 2018 Apr;129(4):783-786. doi: 10.1016/j.clinph.2018.01.058. Epub 2018 Feb 3. Clin Neurophysiol. 2018. PMID: 29448152
-
[The correlation between the type of positivity of the tilt test and a simultaneous electroencephalogram: the preliminary results].Ital Heart J Suppl. 2000 Jan;1(1):103-9. Ital Heart J Suppl. 2000. PMID: 10832126 Italian.
-
Inadequate sympathovagal balance in response to orthostatism in patients with unexplained syncope and a positive head up tilt test.Heart. 1999 Sep;82(3):312-8. doi: 10.1136/hrt.82.3.312. Heart. 1999. PMID: 10455081 Free PMC article.
-
[Syncope of undetermined nature after electrophysiologic study. Usefulness of the head-up tilt test in the diagnosis of vaso-vagal origin and in the choice of treatment].G Ital Cardiol. 1990 Mar;20(3):185-94. G Ital Cardiol. 1990. PMID: 1971602 Review. Italian.
-
Can serial tilt testing be used to evaluate therapy in neurally mediated syncope?Am J Cardiol. 1996 Mar 1;77(7):521-3. doi: 10.1016/s0002-9149(97)89348-4. Am J Cardiol. 1996. PMID: 8629595 Review.
Cited by
-
Diagnosis and prevention of the vasodepressor type of neurally mediated syncope in Japanese patients.PLoS One. 2021 Jun 25;16(6):e0251450. doi: 10.1371/journal.pone.0251450. eCollection 2021. PLoS One. 2021. PMID: 34170907 Free PMC article.
-
Vasovagal syncope interrupting sleep?Heart. 2004 May;90(5):e25. doi: 10.1136/hrt.2003.031294. Heart. 2004. PMID: 15084573 Free PMC article.
-
Pathophysiology of syncope.Clin Auton Res. 2004 Oct;14 Suppl 1:18-24. doi: 10.1007/s10286-004-1004-2. Clin Auton Res. 2004. PMID: 15480926 Review.
-
Near infrared spectroscopy: guided tilt table testing for syncope.Pediatr Cardiol. 2010 Jul;31(5):674-9. doi: 10.1007/s00246-010-9683-z. Epub 2010 Mar 4. Pediatr Cardiol. 2010. PMID: 20204346
-
Association of adenylate cyclase activity in vasopressor-type neurally mediated syncope based on the α2b-AR gene.PLoS One. 2025 Feb 3;20(2):e0317817. doi: 10.1371/journal.pone.0317817. eCollection 2025. PLoS One. 2025. PMID: 39899602 Free PMC article.
References
-
- Morillo C, Ellenbogen KA, Fernando Pava L. Pathophysiologic basis for vasodepressor syncope. Cardiol Clin 1997;15:233–49. - PubMed
-
- Abboud F. Neurocardiogenic syncope. N Engl J Med 1993;328:1117–9. - PubMed
-
- Mark A. The Bezold-Jarisch reflex revisited: clinical implications of inhibitory reflexes originating in the heart. J Am Coll Cardiol 1983;1:90–102. - PubMed
-
- Novak V, Honos G, Schondorf R. Is the heart empty at syncope? J Auton Nerv Syst 1996;60:83–92. - PubMed
-
- Liu J, Hahn RT, Stein M, et al. Left ventricular geometry and function proceeding neurally mediated syncope. Circulation 2000;101:777–91. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous