

Review
doi: 10.1136/heart.88.3.298.
Acute myocardial infarction: reperfusion treatment
Affiliations
- PMID: 12181231
- PMCID: PMC1767333
- DOI: 10.1136/heart.88.3.298
Item in Clipboard
Review
Acute myocardial infarction: reperfusion treatment
Heart.
2002 Sep.
No abstract available
Figures
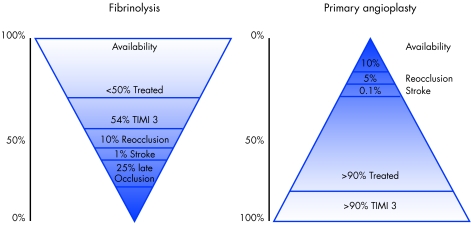
Nearly all patients with acute myocardial infarction (AMI) could potentially benefit from reperfusion treatment with fibrinolytics, but less than 50% will actually be treated; only 50–60% of those will achieve a TIMI 3 grade coronary flow, 10% will suffer from early reocclusion, 1% will have a stroke, and 20–30% will have late reocclusion. On the other hand, angioplasty can be offered to only 10% of patients with AMI, but more than 90% of these will actually be treated; 90% will achieve a TIMI 3 grade coronary flow, less than 5% will have reocclusion, and less than 0.1% will have a stroke.
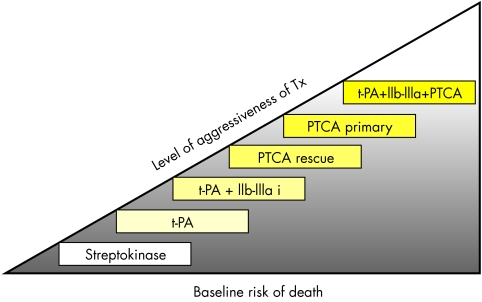
Streptokinase can still be used as a first choice treatment in low risk patients (as currently done in many patients treated in South America, UK, Australia, New Zealand, and the Netherlands), while patients presenting with higher clinical risk would benefit from the use of the more expensive recombinant tissue plasminogen activator (t-PA). The combination of recombinant t-PA and a glycoprotein IIb/IIIa inhibitor (abciximab) will reduce the clinical complications of acute myocardial infarction, but will not reduce mortality. Rescue angioplasty (PTCA) can be reserved for high risk patients who did not achieve reperfusion or have a poor clinical course. Primary angioplasty should be preferred for patients presenting with haemodynamic failure, advanced age (> 75 years) or presenting late (more than 4–5 hours after symptom onset). The previous administration of half doses of lytic treatment is desirable when it can be given out of hospital by first aid providers, or in the emergency department when access to the catheterisation laboratory is delayed. The use of stents and glycoprotein IIb/IIIa inhibitors during angioplasty does not reduce mortality. Instead of being used indiscriminately, these tools should be considered in unfavourable patient or lesion subsets, such as in the presence of a large thrombotic burden after wire crossing or suboptimal flow after angioplasty.
References
-
- Antman EM, Giugliano RP, Gibson CM, et al for the TIMI 14 Investigators. Abciximab facilitates the rate and extent of thrombolysis: results of the thrombolysis in myocardial infarction (TIMI) 14 trial. Circulation 1999;99:2720–32. - PubMed
-
- Brener SJ, Barr LA, Burchenal J, et al. Randomized, placebo-controlled trial of platelet glycoprotein IIb-IIIa blockade with primary angioplasty for acute myocardial infarction. The RAPPORT trial. Circulation 1998;98:734–41 - PubMed
-
- Ross AM, Coyne KS, Reiner JS, et al for the PACT Investigators. A randomized trial comparing primary angioplasty with a strategy of short-acting thrombolysis and immediate planned rescue angioplasty in acute myocardial infarction: the PACT trial. J Am Coll Cardiol 1999;34:1954–62. - PubMed
-
- Franzosi MG, Santoro E, De Vita C, et al, on behalf of the GISSI Investigators. Ten-year follow-up of the first megatrial testing thrombolytic therapy in patients with acute myocardial infarction. Circulation 1998;98:2659–65. - PubMed
-
- GUSTO Investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med 1993;329:673–82. Large reperfusion trial that showed a significant (14.6%) risk reduction in mortality with rt-PA and heparin compared to streptokinase. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical