

Emmetropisation following preterm birth
- PMID: 12185134
- PMCID: PMC1771279
- DOI: 10.1136/bjo.86.9.1035
Emmetropisation following preterm birth
Abstract
Background/aims: Even in the absence of retinopathy of prematurity (ROP), premature birth signals increased risk for abnormal refractive development. The present study examined the relation between clinical risk factors and refractive development among preterm infants without ROP.
Methods: Cycloplegic refraction was measured at birth, term, 6, 12, and 48 months corrected age in a cohort of 59 preterm infants. Detailed perinatal history and cranial ultrasound data were collected. 40 full term (plus or minus 2 weeks) subjects were tested at birth, 6, and 12 months old.
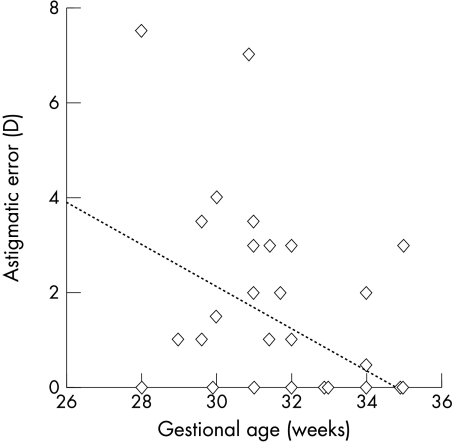
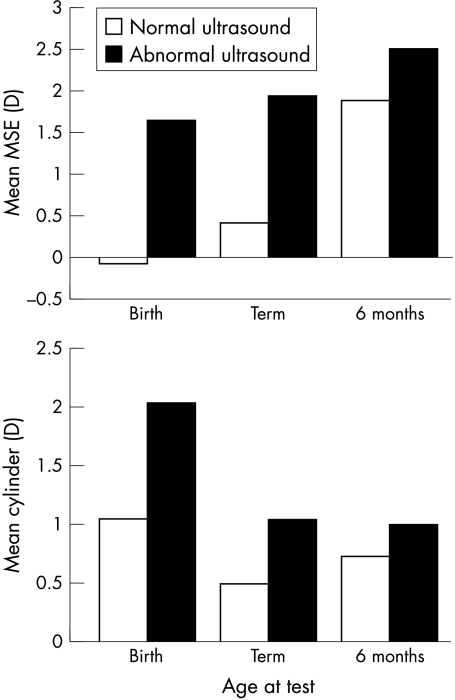
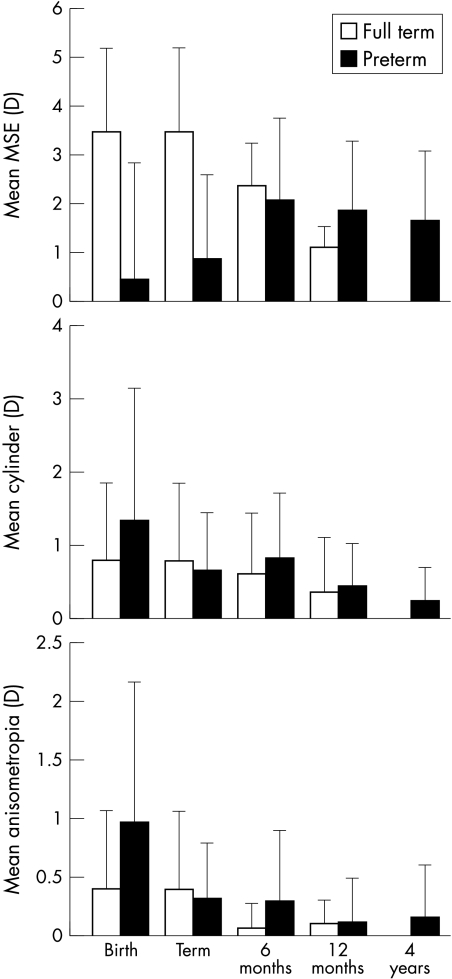
Results: Myopia and anisometropia were associated with prematurity (p<0.05). More variation in astigmatic axis was found among preterm infants (p<0.05) and a trend for more astigmatism (p<0.1). Emmetropisation occurred in the preterm infants so that at term age they did not differ from the fullterm group in astigmatism or anisometropia. However, preterm infants remained more myopic (less hyperopic) than the fullterm group at term (p<0.05) and those infants born <1500 g remained more anisometropic than their peers until 6 months (p<0.05). Infants with abnormal cranial ultrasound were at risk for higher hyperopia (p<0.05). Other clinical risk factors were not associated with differences in refractive development. At 4 years of age 19% of the preterm group had clinically significant refractive errors.
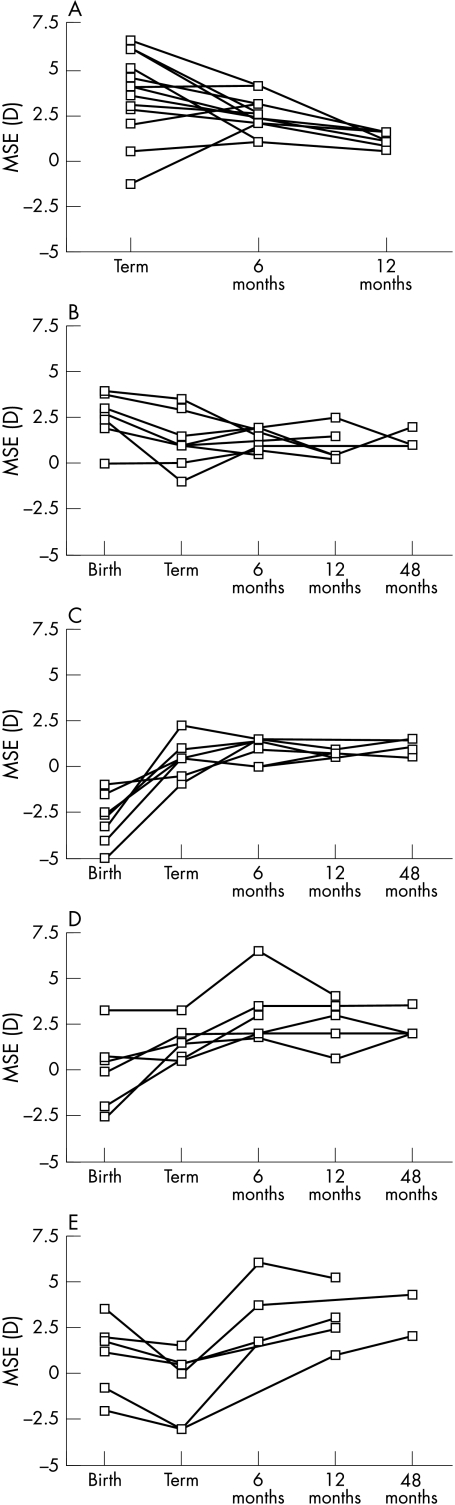
Conclusion: Preterm infants without ROP had high rates of refractive error. The early emmetropisation process differed from that of the fullterm group but neither clinical risk factors nor measures of early refractive error were predictive of refractive outcome at 4 years.
Figures
Similar articles
-
Ophthalmological long-term follow up of preterm infants: a population based, prospective study of the refraction and its development.Br J Ophthalmol. 1998 Nov;82(11):1265-71. doi: 10.1136/bjo.82.11.1265. Br J Ophthalmol. 1998. PMID: 9924330 Free PMC article.
-
Refractive outcome of premature infants with or without retinopathy of prematurity at 2 years of age: a prospective controlled cohort study.Kaohsiung J Med Sci. 2012 Apr;28(4):204-11. doi: 10.1016/j.kjms.2011.10.010. Epub 2012 Feb 12. Kaohsiung J Med Sci. 2012. PMID: 22453068 Free PMC article.
-
Refractive Status in Nepalese Pre-Term and Full-Term Infants Early in Life.Optom Vis Sci. 2017 Oct;94(10):957-964. doi: 10.1097/OPX.0000000000001118. Optom Vis Sci. 2017. PMID: 28858003
-
Ocular sequelae in premature infants.Pediatrics. 1993 Dec;92(6):787-90. Pediatrics. 1993. PMID: 8233737 Review.
-
Development of refractive error in children treated for retinopathy of prematurity with anti-vascular endothelial growth factor (anti-VEGF) agents: A meta-analysis and systematic review.PLoS One. 2019 Dec 2;14(12):e0225643. doi: 10.1371/journal.pone.0225643. eCollection 2019. PLoS One. 2019. PMID: 31790445 Free PMC article.
Cited by
-
Evaluation of Ocular Biometric and Optical Coherence Tomography Parameters in Preterm Children Without Retinopathy of Prematurity.Transl Vis Sci Technol. 2022 Mar 2;11(3):8. doi: 10.1167/tvst.11.3.8. Transl Vis Sci Technol. 2022. PMID: 35258558 Free PMC article.
-
Interocular Difference of Peripheral Refraction in Anisomyopic Eyes of Schoolchildren.PLoS One. 2016 Feb 16;11(2):e0149110. doi: 10.1371/journal.pone.0149110. eCollection 2016. PLoS One. 2016. PMID: 26881745 Free PMC article.
-
Anisometropia in children from infancy to 15 years.Invest Ophthalmol Vis Sci. 2012 Jun 20;53(7):3782-7. doi: 10.1167/iovs.11-8727. Invest Ophthalmol Vis Sci. 2012. PMID: 22589429 Free PMC article.
-
Associations Between Fetal Growth Trajectories and the Development of Myopia by 20 Years of Age.Invest Ophthalmol Vis Sci. 2020 Dec 1;61(14):26. doi: 10.1167/iovs.61.14.26. Invest Ophthalmol Vis Sci. 2020. PMID: 33355605 Free PMC article.
-
Results of extremely-low-birth-weight infants randomized to receive extra enteral calcium supply.J Pediatr Gastroenterol Nutr. 2011 Sep;53(3):339-45. doi: 10.1097/MPG.0b013e3182187ecd. J Pediatr Gastroenterol Nutr. 2011. PMID: 21865980 Free PMC article. Clinical Trial.
References
-
- Fletcher MC, Brandon S. Myopia of prematurity. Am J Ophthalmol 1955;40:474–81. - PubMed
-
- Shapiro A, Yanko L, Nawratzki I, et al. Refractive power of premature children at infancy and early childhood. Am J Ophthalmol 1980;90:234–8. - PubMed
-
- Dobson V, Fulton AB, Manning K, et al. Cycloplegic refractions of premature infants. Am J Ophthalmol 1981;91:490–5. - PubMed
-
- Gordon RA, Donzis PB. Myopia associated with retinopathy of prematurity. Ophthalmology 1986;93:1593–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical