

The effects of cost-sharing on essential drug prescriptions, utilization of medical care and outcomes after acute myocardial infarction in elderly patients
- PMID: 12186169
- PMCID: PMC117469
The effects of cost-sharing on essential drug prescriptions, utilization of medical care and outcomes after acute myocardial infarction in elderly patients
Abstract
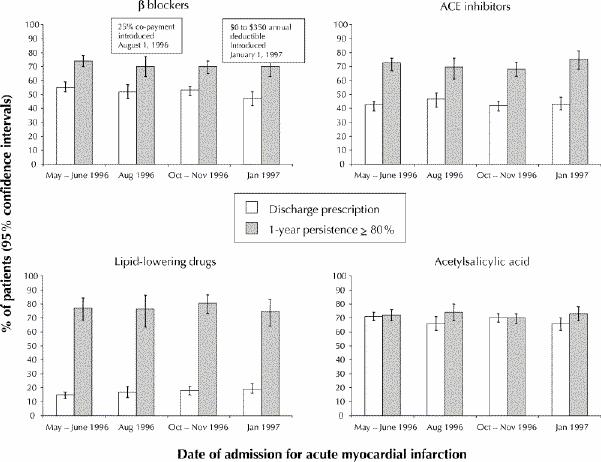
Background: After a change in Quebec's policy on drug coverage in August 1996, elderly patients' copayments for prescription drugs increased. We assessed the impact of this drug policy reform on prescribing patterns for essential cardiac medications, utilization of medical care and related health outcomes after acute myocardial infarction.
Methods: Patients at least 65 years of age who experienced acute myocardial infarction between 1994 and 1998 were identified through the Quebec discharge summary database. Drug claims databases were analyzed to determine rates of prescription of essential cardiac medications for cohorts of patients admitted before and after the policy reform. The impact on readmissions for cardiac-related complications, outpatient visits to physicians and emergency departments, and mortality rate was also assessed.
Results: The proportion of patients who received prescriptions for beta-blockers, angiotensin-converting enzyme inhibitors and lipid-lowering drugs increased over time and, more specifically, did not appear to decline with the change in the drug policy. In addition, the policy reform did not appear to affect persistence of drug therapy (the proportion of time for which patients were covered by prescriptions over the year after discharge). There was no within-class shift from more to less expensive drugs. Use of cardiac procedures increased over time, but this increase was unrelated to the date of the policy reform. Finally, rates of readmission for complications, visits to individual physicians and to emergency departments, and mortality rate were unchanged. The findings did not vary with sex or socioeconomic status.
Interpretation: Prescriptions for essential cardiac medications and care related to acute myocardial infarction in elderly patients did not change with increases in out-of-pocket copayment, regardless of sex or socioeconomic status.
Figures
Similar articles
-
Assessing the effect of Taiwan's outpatient prescription drug copayment policy in the elderly.Med Care. 2003 Dec;41(12):1331-42. doi: 10.1097/01.MLR.0000100579.91550.C4. Med Care. 2003. PMID: 14668666
-
Outcomes of reference pricing for angiotensin-converting-enzyme inhibitors.N Engl J Med. 2002 Mar 14;346(11):822-9. doi: 10.1056/NEJMsa003087. N Engl J Med. 2002. PMID: 11893794
-
Drug prescriptions after acute myocardial infarction: dosage, compliance, and persistence.Am Heart J. 2003 Mar;145(3):438-44. doi: 10.1067/mhj.2003.143. Am Heart J. 2003. PMID: 12660666
-
[Management of acute myocardial infarction in the experience of a community hospital. A prospective study].Minerva Cardioangiol. 1997 Jul-Aug;45(7-8):335-47. Minerva Cardioangiol. 1997. PMID: 9463169 Review. Italian.
-
AT1 receptor blockade for the prevention of cardiovascular events after myocardial infarction.Expert Rev Cardiovasc Ther. 2004 Nov;2(6):891-902. doi: 10.1586/14779072.2.6.891. Expert Rev Cardiovasc Ther. 2004. PMID: 15500434 Review.
Cited by
-
The effects of patient cost-sharing on health expenditure and health among older people: Heterogeneity across income groups.Eur J Health Econ. 2022 Jul;23(5):847-861. doi: 10.1007/s10198-021-01399-6. Epub 2021 Nov 15. Eur J Health Econ. 2022. PMID: 34779932 Free PMC article.
-
How patient cost-sharing trends affect adherence and outcomes: a literature review.P T. 2012 Jan;37(1):45-55. P T. 2012. PMID: 22346336 Free PMC article.
-
The Influence of National Health Insurance on Medication Adherence Among Outpatient Type 2 Diabetics in Southwest Nigeria.J Patient Exp. 2018 Jun;5(2):114-119. doi: 10.1177/2374373517732384. Epub 2017 Sep 29. J Patient Exp. 2018. PMID: 29978027 Free PMC article.
-
How does copayment for health care services affect demand, health and redistribution? A systematic review of the empirical evidence from 1990 to 2011.Eur J Health Econ. 2014 Nov;15(8):813-28. doi: 10.1007/s10198-013-0526-8. Epub 2013 Aug 29. Eur J Health Econ. 2014. PMID: 23989938
-
Review of evidence and explanations for suboptimal screening and treatment of dyslipidemia in women. A conceptual model.J Gen Intern Med. 2003 Oct;18(10):854-63. doi: 10.1046/j.1525-1497.2003.20910.x. J Gen Intern Med. 2003. PMID: 14521649 Free PMC article. Review.
References
-
- Pilote L, Lavoie F, Ho V, Eisenberg MJ. Changes in the treatment of acute myocardial infarction in Quebec, 1988–1995. CMAJ 2000;163:31-6. Available: www.cmaj.ca/cgi/content/full/163/1/31. - PMC - PubMed
-
- Stuart B, Zacker C. Who bears the burden of Medicaid drug copayment policies? Health Aff (Millwood) 1999;18:201-12. - PubMed
-
- Levy RA, Tamblyn R, Fitchett D, McLeod P, Hanley JA. Coding accuracy of hospital discharge for elderly survivors of myocardial infarction. Can J Cardiol 1999;15:1277-82. - PubMed
-
- Tamblyn R, Lavoie G, Petrella L, Monette J. The use of prescription claims databases in pharmacoepidemiological research: the accuracy and comprehensiveness of the prescription claims databases in Quebec. J Clin Epidemiol 1995;48:999-1009. - PubMed
-
- Ryan TJ, Anderson JL, Antman EM, Braniff BA, Brooks NH, Califf RM, et al. ACC/AHA guidelines for the management of patients with acute myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infarction). J Am Coll Cardiol 1996;28:1328-428. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical