

Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality
- PMID: 12192322
- PMCID: PMC1422589
- DOI: 10.1097/00000658-200209000-00012
Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality
Abstract
Objective: To evaluate, in a prospective, randomized single-institution trial, the end points of operative morbidity, operative mortality, and survival in patients undergoing standard versus radical (extended) pancreaticoduodenectomy.
Summary background data: Numerous retrospective reports and a few prospective randomized trials have suggested that the performance of an extended lymphadenectomy in association with a pancreaticoduodenal resection may improve survival for patients with pancreatic and other periampullary adenocarcinomas.
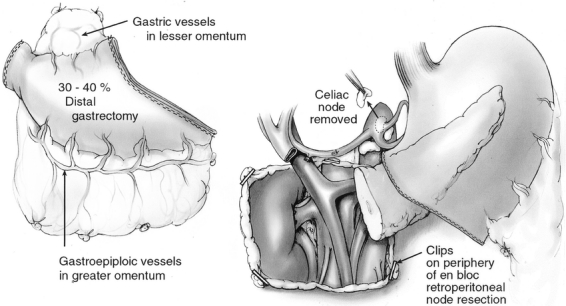
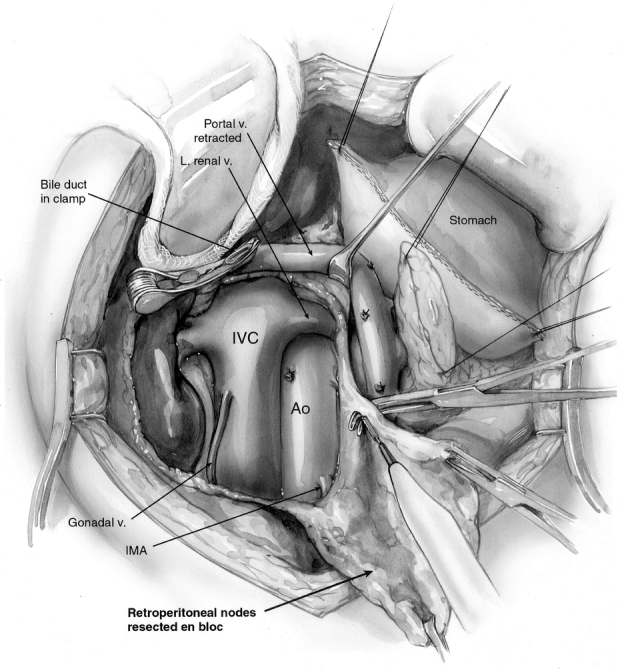
Methods: Between April 1996 and June 2001, 299 patients with periampullary adenocarcinoma were enrolled in a prospective, randomized single-institution trial. After intraoperative verification (by frozen section) of margin-negative resected periampullary adenocarcinoma, patients were randomized to either a standard pancreaticoduodenectomy (removing only the peripancreatic lymph nodes en bloc with the specimen) or a radical (extended) pancreaticoduodenectomy (standard resection plus distal gastrectomy and retroperitoneal lymphadenectomy). All pathology specimens were reviewed, fully categorized, and staged. The postoperative morbidity, mortality, and survival data were analyzed.
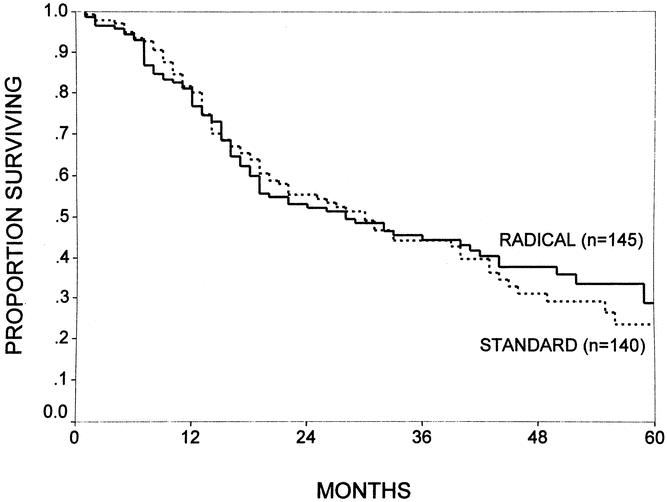
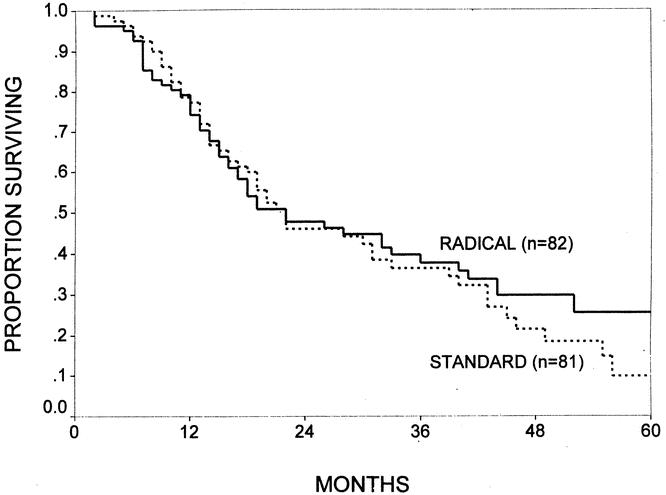
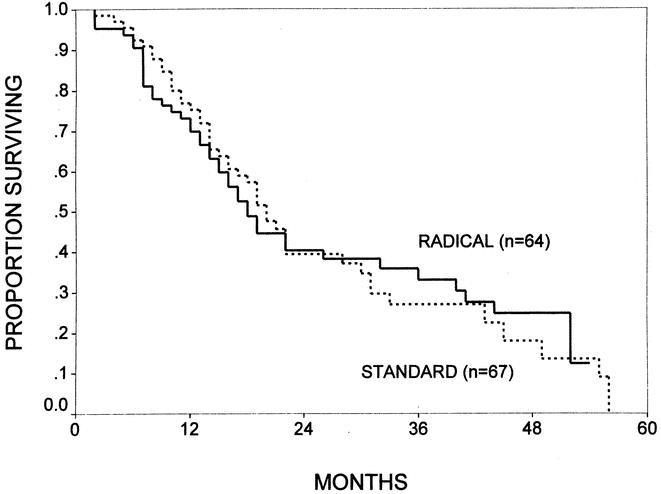
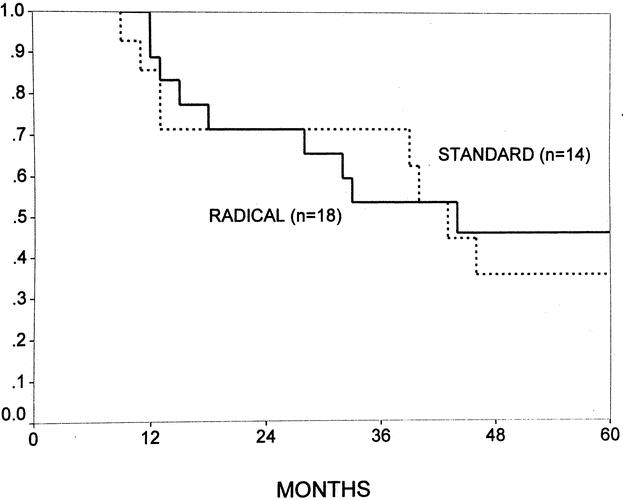
Results: Of the 299 patients randomized, 5 (1.7%) were subsequently excluded because their final pathology failed to reveal periampullary adenocarcinoma, leaving 294 patients for analysis (146 standard vs. 148 radical). The two groups were statistically similar with regard to age (median 67 years) and gender (54% male). All the patients in the radical group underwent distal gastric resection, while 86% of the patients in the standard group underwent pylorus preservation ( <.0001). The mean operative time in the radical group was 6.4 hours, compared to 5.9 hours in the standard group ( =.002). There were no significant differences between the two groups with respect to intraoperative blood loss, transfusion requirements (median zero units), location of primary tumor (57% pancreatic, 22% ampullary, 17% distal bile duct, 3% duodenal), mean tumor size (2.6 cm), positive lymph node status (74%), or positive margin status on final permanent section (10%). The mean total number of lymph nodes resected was significantly higher in the radical group. Of the 148 patients in the radical group, only 15% (n = 22) had metastatic adenocarcinoma in the resected retroperitoneal lymph nodes, and none had retroperitoneal nodes as the only site of lymph node involvement. One patient in the radical group with negative pancreaticoduodenectomy specimen lymph nodes had a micrometastasis to one perigastric lymph node. There were six perioperative deaths (4%) in the standard group versus three perioperative deaths (2%) in the radical group ( = NS). The overall complication rates were 29% for the standard group versus 43% for the radical group ( =.01), with patients in the radical group having significantly higher rates of early delayed gastric emptying and pancreatic fistula and a significantly longer mean postoperative stay. With a mean patient follow-up of 24 months, there were no significant differences in 1-, 3-, or 5-year and median survival when comparing the standard and radical groups.
Conclusions: Radical (extended) pancreaticoduodenectomy can be performed with similar mortality but some increased morbidity compared to standard pancreaticoduodenectomy. The data to date fail to indicate that a survival benefit is derived from the addition of a distal gastrectomy and retroperitoneal lymphadenectomy to a pylorus-preserving pancreaticoduodenectomy.
Figures
References
-
- Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg 1993; 165: 68–73. - PubMed
-
- Delcore R, Rodriquez FJ, Forster J, et al. Significance of lymph node metastases in patients with pancreatic cancer undergoing curative resection. Am J Surg 1996; 172: 463–469. - PubMed
-
- Yeo CJ, Cameron JL. Review topic: Prognostic factors in ductal pancreatic cancer. Langenbeck’s Arch Surg 1998; 383: 129–133. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
