

Treatment outcomes of resected esophageal cancer
- PMID: 12192324
- PMCID: PMC1422591
- DOI: 10.1097/00000658-200209000-00014
Treatment outcomes of resected esophageal cancer
Abstract
Objective: To assess the evolution of treatment and outcome for resected esophageal cancer at a single institution.
Summary background data: Strategies for optimizing the treatment of resected esophageal cancer continue to evolve over time. The outcomes of these evolving treatments in the context of improved diagnostic staging and changing epidemiology have not been carefully analyzed in a single institution.
Methods: One thousand ninety-seven consecutive patients with primary esophageal cancer underwent surgery during the period 1970 to 2001. Nine hundred ninety-four patients underwent curative esophagectomy and were analyzed for changing demographics. Eight hundred seventy-nine patients who did not have systemic metastases and survived the perioperative period were assessed by multivariate analysis for factors associated with long-term survival.
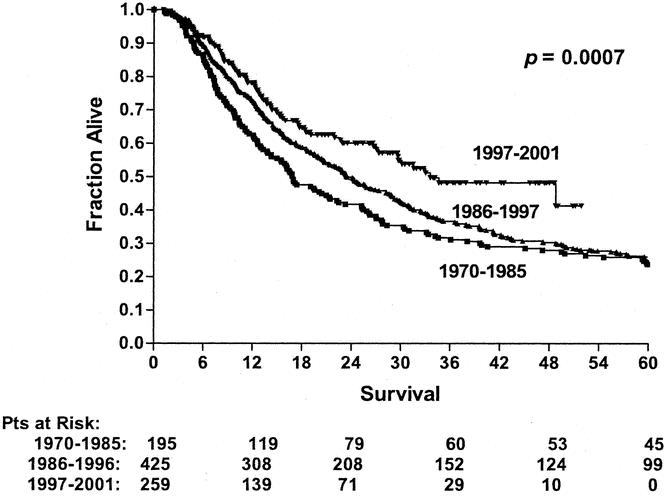
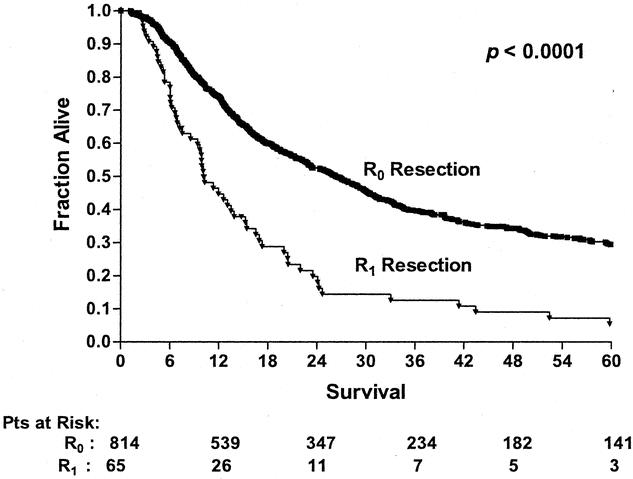
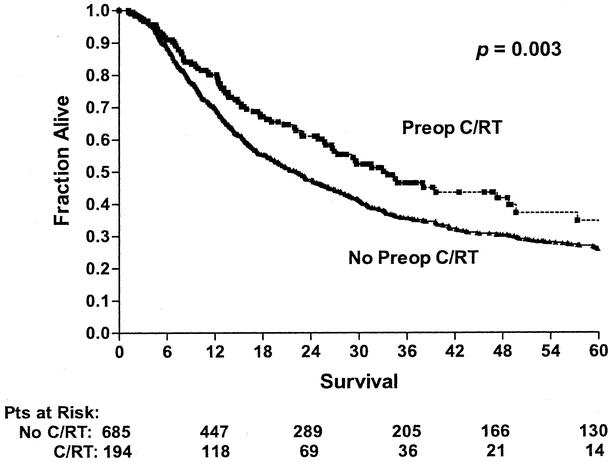
Results: During the study period the overall median survival increased from 17 to 34 months, and combined hospital and 30-day mortality decreased from 12% to 6%. The R0 resection rate increased from 78 to 94%, and adenocarcinoma replaced squamous cell carcinoma as the predominant histology (83% vs. 17%). No change in survival with time was noted for patients treated with surgery alone having the same postoperative pathologic stage (pTNM). An increased proportion of patients had preoperative chemoradiation in the last 4 years of the study (59% vs. 2%). Preoperative chemoradiation was associated with a longer survival and increased likelihood of achieving a complete resection. Multivariate analysis showed that long-term survival was associated with a complete resection and the preoperative staging strategy used, while the use of preoperative chemoradiation was the most significant factor associated with ability to achieve an R0 esophageal resection.
Conclusions: This study shows favorable trends in the survival of patients with resected esophageal cancer over time. The increased use of preoperative chemoradiation, better preoperative staging, and other time-dependent factors may have contributed to the observed increase in survival.
Figures
References
-
- Swisher SG, Hunt KK, Holmes EC, et al. Changes in the surgical management of esophageal cancer from 1970 to 1993. Am J Surg 1995; 169: 609–614. - PubMed
-
- Blot WJ, Devesa SS, Kneller RW, et al. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 1991; 265: 1287–1289. - PubMed
-
- Swisher SG, Holmes EC, Hunt, et al. The role of neoadjuvant therapy in surgically resectable esophageal cancer. Arch Surg 1996; 131: 819–825. - PubMed
-
- Muller J, Erasmi H, Stelzner M, et al. Surgical therapy of oesophageal carcinoma. Br J Surg 1990; 77: 845–857. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
