

Activation of pulmonary T cells in corticosteroid-resistant and -sensitive interstitial pneumonitis in dermatomyositis/polymyositis
- PMID: 12197897
- PMCID: PMC1906473
- DOI: 10.1046/j.1365-2249.2002.01933.x
Activation of pulmonary T cells in corticosteroid-resistant and -sensitive interstitial pneumonitis in dermatomyositis/polymyositis
Abstract
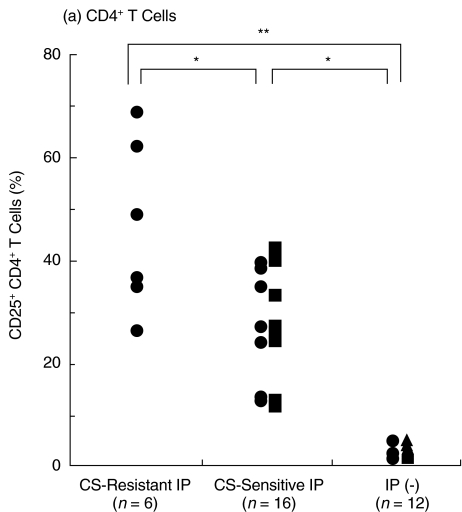
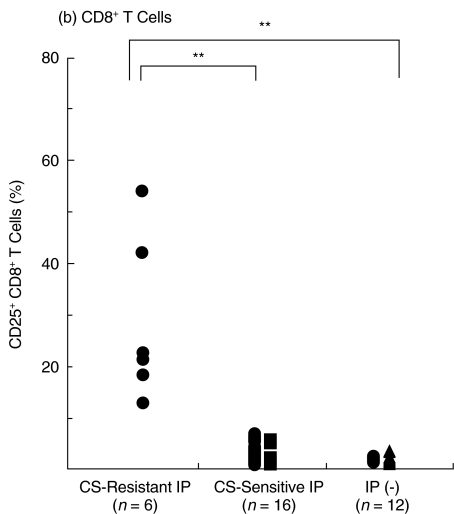
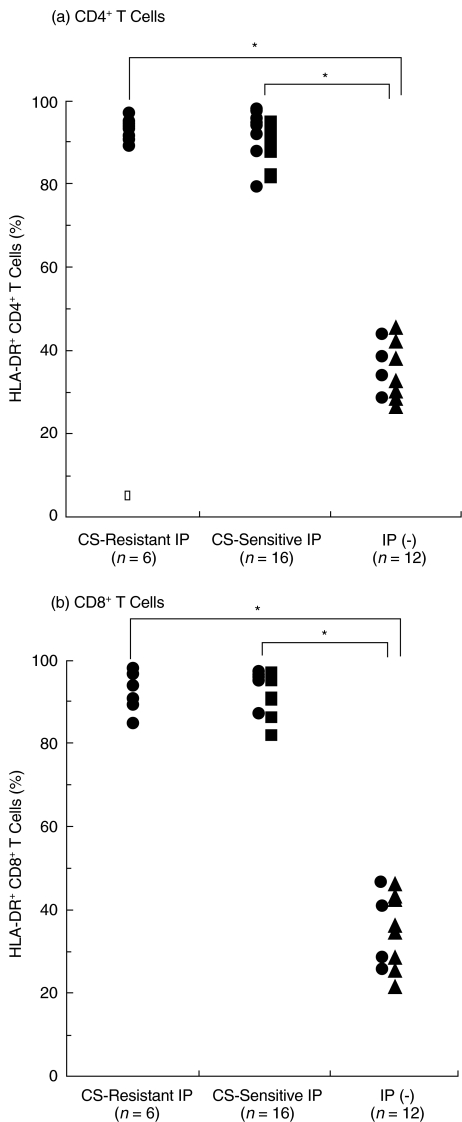
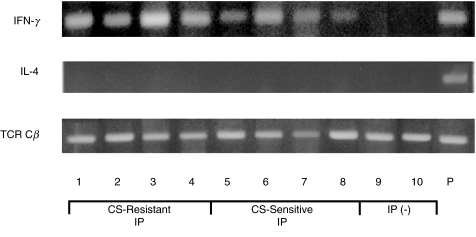
To study the activation states and cytokine profiles of pulmonary T cells in corticosteroid-resistant and corticosteroid-sensitive interstitial pneumonitis (IP) in dermatomyositis (DM)/polymyositis (PM), we examined the activation markers and cytokine profiles of T cells in bronchoalveolar lavage fluids (BALF) from patients with IP in DM/PM before prednisolone therapy and then compared the activation states of T cells according to the therapeutic response of IP to prednisolone therapy. CD25+ CD4+ T cells in BALF were significantly increased in both corticosteroid-resistant and corticosteroid-sensitive IP in DM/PM as compared with those in controls without IP. Furthermore, CD25+ CD4+ T cells in BALF were significantly more increased in corticosteroid-resistant IP than those in cortico teroid- sensitive IP. Moreover, CD25+ CD8+ T cells in BALF were significantly increased only in corticosteroid-resistant IP, but not in corticosteroid-sensitive IP or controls without IP. IFN-gamma mRNA was detected in BALF T cells in corticosteroid-resistant and corticosteroid-sensitive IP but not in controls without IP, whereas IL-4 mRNA was virtually undetected in BALF T cells in both the IP groups. However, there were no significant differences in CD4/CD8 ratio of BALF T cells, HLA-DR+ BALF T cells or CD25+ and HLA-DR+ peripheral blood T cells between the two IP groups. These results indicate that activated Th1-type pulmonary T cells play an important role in the development of corticosteroid- resistant IP in DM/PM and that the increase in CD25+ CD8+ T cells in BALF is a useful indicator for corticosteroid-resistant IP in DM/PM and hence may be an indicator for early use of cyclosporin.
Figures
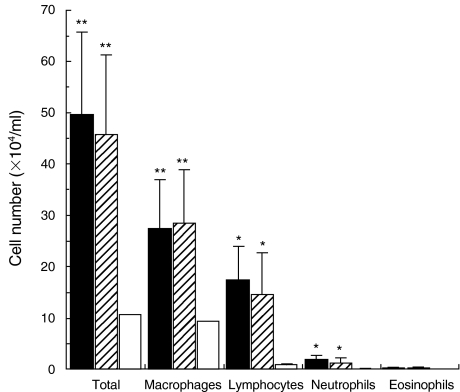
 ) and from controls without IP including DM patients without IP (n = 12, □), and the number of total cells, lymphocytes, macrophages, neutrophils, and eosinophils in BALF was evaluated. Data are means ± SD in each group. Significant different from the mean values in controls without IP, *P < 0·05, **P < 0·005.
) and from controls without IP including DM patients without IP (n = 12, □), and the number of total cells, lymphocytes, macrophages, neutrophils, and eosinophils in BALF was evaluated. Data are means ± SD in each group. Significant different from the mean values in controls without IP, *P < 0·05, **P < 0·005.
Similar articles
-
Corticosteroid resistant interstitial pneumonitis in dermatomyositis/polymyositis: prediction and treatment with cyclosporine.J Rheumatol. 1999 Jul;26(7):1527-33. J Rheumatol. 1999. PMID: 10405940
-
T cell receptor BV gene repertoire of lymphocytes in bronchoalveolar lavage fluid of polymyositis/dermatomyositis patients with interstitial pneumonitis.Int J Mol Med. 2006 Jan;17(1):101-9. Int J Mol Med. 2006. PMID: 16328018
-
T-cell activation profiles in different granulomatous interstitial lung diseases--a role for CD8+CD28(null) cells?Clin Exp Immunol. 2010 May;160(2):256-65. doi: 10.1111/j.1365-2249.2009.04076.x. Epub 2009 Dec 17. Clin Exp Immunol. 2010. PMID: 20030671 Free PMC article.
-
Polymyositis/dermatomyositis and interstitial lung disease: a new therapeutic approach with T-cell-specific immunosuppressants.Autoimmunity. 2005 Aug;38(5):383-92. doi: 10.1080/08916930500124023. Autoimmunity. 2005. PMID: 16227154 Review.
-
[Deep lung--cellular reaction to HIV].Rev Port Pneumol. 2007 Mar-Apr;13(2):175-212. Rev Port Pneumol. 2007. PMID: 17492233 Review. Portuguese.
Cited by
-
Survival benefit associated with early cyclosporine treatment for dermatomyositis-associated interstitial lung disease.Rheumatol Int. 2016 Jan;36(1):125-31. doi: 10.1007/s00296-015-3328-8. Epub 2015 Jul 30. Rheumatol Int. 2016. PMID: 26223808
-
Coadministration of cyclosporin a with prednisolone in acute interstitial pneumonia complicating polymyositis/dermatomyositis.Clin Med Insights Arthritis Musculoskelet Disord. 2012;5:43-52. doi: 10.4137/CMAMD.S9398. Epub 2012 Mar 14. Clin Med Insights Arthritis Musculoskelet Disord. 2012. PMID: 22442637 Free PMC article.
-
Early assessment of rapidly progressive interstitial pneumonia associated with amyopathic dermatomyositis.Clin Rheumatol. 2007 Mar;26(3):436-9. doi: 10.1007/s10067-005-0147-4. Epub 2005 Dec 20. Clin Rheumatol. 2007. PMID: 16365687
-
Increased Serum LIGHT Levels Correlate with Disease Progression and Severity of Interstitial Pneumonia in Patients with Dermatomyositis: A Case Control Study.PLoS One. 2015 Oct 8;10(10):e0140117. doi: 10.1371/journal.pone.0140117. eCollection 2015. PLoS One. 2015. PMID: 26448572 Free PMC article.
-
Phenotypes of Peripheral Blood Lymphocytes and Cytokine Expression in Polymyositis and Dermatomyositis before Treatment and after Clinical Remission.Clin Med Insights Arthritis Musculoskelet Disord. 2012;5:77-87. doi: 10.4137/CMAMD.S10272. Epub 2012 Oct 18. Clin Med Insights Arthritis Musculoskelet Disord. 2012. PMID: 23115480 Free PMC article.
References
-
- Frazier AR, Miller RD. Interstitial pneumonitis in association with polymyositis and dermatomyositis. Chest. 1974;65:403–7. - PubMed
-
- Songcharoen S, Raju SF, Pennebaker JB. Interstitial lung disease in polymyositis and dermatomyositis. J Rheumatol. 1980;7:353–60. - PubMed
-
- Salmeron G, Greenberg SD, Lidsky MD. Polymyositis and diffuse interstitial lung disease. Arch Intern Med. 1981;141:1005–10. - PubMed
-
- Dickey BF, Myers AR. Pulmonary disease in polymyositis/ dermatomyositis. Semin Arthritis Rheum. 1984;14:60–76. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
