

Double-blind study to evaluate flow cytometry analysis of anti-live trypomastigote antibodies for monitoring treatment efficacy in cases of human Chagas' disease
- PMID: 12204967
- PMCID: PMC120067
- DOI: 10.1128/cdli.9.5.1107-1113.2002
Double-blind study to evaluate flow cytometry analysis of anti-live trypomastigote antibodies for monitoring treatment efficacy in cases of human Chagas' disease
Abstract
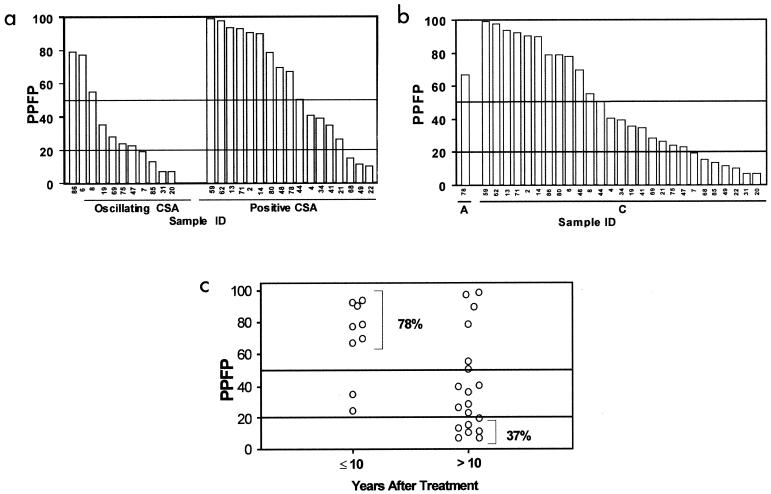
The validation of flow cytometry analysis of anti-live trypomastigote antibodies (FC-ALTA) to monitor cure after treatment of Chagas' disease was evaluated with serum samples from treated and nontreated chagasic patients. After optimization of the original technique, toward better sensitivity and applicability to field surveys, we design a double blind study of 94 coded samples classified into the following categories: patients not treated (NT) and patients treated but not cured (TNC), both presenting positive conventional serology and xenodiagnosis; patients treated and cured (TC), showing negative serology and xenodiagnosis; and patients treated under evaluation (TUE), who presented positive or oscillating conventional serology (CSA) but negative xenodiagnosis. Coded samples, diluted 1:256, were assayed by incubation with live cell culture trypomastigotes, which were subsequently stained with fluorescein isothiocyanate-conjugated anti-human immunoglobulin G, with prior fixation and analysis by flow cytometry. The results were expressed as the percentages of positive fluorescent parasites (PPFP) for each individual sample, establishing 20% PPFP as the cutoff between negative and positive results. Our data demonstrated that all NT and TNC presented positive results while all but one TC had a PPFP lower than 20%. Analysis of TUE demonstrated a wide degree of reactivity, with PPFP values that were negative (PPFP </= 20%), low positive (20% < PPFP </= 50%), and high positive (PPFP > 50%). As TUE with negative PPFP presented negative xenodiagnosis and positive or oscillating CSA, they were classified as dissociated according to the criteria of Krettli and Brener (J. Immunol. 128:2009-2012, 1982) and could indeed be considered cured after chemotherapy. This study demonstrates and validates the use of FC-ALTA to easily identify anti-live trypomastigote membrane-bound antibodies, offering another approach for investigating and monitoring the efficacy of specific chemotherapy in cases of human Chagas' disease.
Figures





Similar articles
-
Innovations in diagnosis and post-therapeutic monitoring of Chagas disease: Simultaneous flow cytometric detection of IgG1 antibodies anti-live amastigote, anti-live trypomastigote, and anti-fixed epimastigote forms of Trypanosoma cruzi.J Immunol Methods. 2014 Nov;413:32-44. doi: 10.1016/j.jim.2014.07.005. Epub 2014 Jul 24. J Immunol Methods. 2014. PMID: 25064148
-
Flow cytometry, a new approach to detect anti-live trypomastigote antibodies and monitor the efficacy of specific treatment in human Chagas' disease.Clin Diagn Lab Immunol. 1995 Sep;2(5):569-73. doi: 10.1128/cdli.2.5.569-573.1995. Clin Diagn Lab Immunol. 1995. PMID: 8548536 Free PMC article.
-
Non-conventional flow cytometry approaches to detect anti-Trypanosoma cruzi immunoglobulin G in the clinical laboratory.J Immunol Methods. 2007 Jan 10;318(1-2):102-12. doi: 10.1016/j.jim.2006.10.009. Epub 2006 Nov 13. J Immunol Methods. 2007. PMID: 17161421
-
[Chagasic megaesophagus with positive serology and xenodiagnosis].Rev Gastroenterol Mex. 1993 Jan-Mar;58(1):36-8. Rev Gastroenterol Mex. 1993. PMID: 8362151 Review. Spanish. No abstract available.
-
Changes in the hemoculture methodology improve the test positivity.Mem Inst Oswaldo Cruz. 1999;94 Suppl 1:295-8. doi: 10.1590/s0074-02761999000700053. Mem Inst Oswaldo Cruz. 1999. PMID: 10677739 Review. No abstract available.
Cited by
-
Parasitological cure and clinical benefits of benznidazole treatment in patients from the Jequitinhonha Valley, MG, Brazil, with recent chronic infection by Trypanosoma cruzi II.Mem Inst Oswaldo Cruz. 2025 Jun 2;120:e240229. doi: 10.1590/0074-02760240229. eCollection 2025. Mem Inst Oswaldo Cruz. 2025. PMID: 40465897 Free PMC article.
-
Oral Chagas disease outbreak by bacaba juice ingestion: A century after Carlos Chagas' discovery, the disease is still hard to manage.PLoS Negl Trop Dis. 2024 Sep 18;18(9):e0012225. doi: 10.1371/journal.pntd.0012225. eCollection 2024 Sep. PLoS Negl Trop Dis. 2024. PMID: 39292716 Free PMC article.
-
A flow cytometry-based workflow for detection and quantification of anti-plasmodial antibodies in vaccinated and naturally exposed individuals.Malar J. 2012 Nov 6;11:367. doi: 10.1186/1475-2875-11-367. Malar J. 2012. PMID: 23130649 Free PMC article. Clinical Trial.
-
Revisiting the Posttherapeutic Cure Criterion in Chagas Disease: Time for New Methods, More Questions, Doubts, and Polemics or Time to Change Old Concepts?Biomed Res Int. 2015;2015:652985. doi: 10.1155/2015/652985. Epub 2015 Oct 25. Biomed Res Int. 2015. PMID: 26583124 Free PMC article. Review.
-
Dissimilar Trypanosoma cruzi genotype-specific serological profile assessed by Chagas-Flow ATE IgG1 upon benznidazole etiological treatment of chronic Chagas disease.PLoS Negl Trop Dis. 2024 Sep 13;18(9):e0012487. doi: 10.1371/journal.pntd.0012487. eCollection 2024 Sep. PLoS Negl Trop Dis. 2024. PMID: 39269987 Free PMC article.
References
-
- Almeida, J. O., J. L. P. Freitas, and H. Brandão. 1954. Complement fixation test with a triple antigen for syphilis, tuberculosis, leprosy or Chagas disease in blood banks. Am. J. Trop. Med. Hyg. 3:490-494. - PubMed
-
- Andrade, Z. A. 1991. Pathogenesis of Chagas' disease. Res. Immunol. 142:126-129. - PubMed
-
- Bertelli, M. S., R. R. Golgher, and Z. Brener. 1977. Intraspecific variation in Trypanosoma cruzi: effect of temperature on the intracellular differentiation in tissue culture. J. Parasitol. 63:434-437. - PubMed
-
- Brener, Z. 1984. Recent advances in the chemotherapy of Chagas' disease. Mem. Inst. Oswaldo Cruz 79(Suppl.):149-155.
-
- Brener, Z., and E. Chiari. 1963. Variações morfológicas observadas em diferentes amostras de Trypanosoma cruzi. Rev. Inst. Med. Trop. Sao Paulo 5:220-224. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
