

Pharmacokinetics and pharmacodynamics of low-dose methotrexate in the treatment of psoriasis
- PMID: 12207634
- PMCID: PMC1874405
- DOI: 10.1046/j.1365-2125.2002.01621.x
Pharmacokinetics and pharmacodynamics of low-dose methotrexate in the treatment of psoriasis
Abstract
Aims: The aim of this 13 week, randomized, parallel-group study was to evaluate the relationship between the pharmacokinetics (PK) and pharmacodynamics (PD) of low-dose intermittent oral methotrexate (LDMTX) in patients with psoriasis.
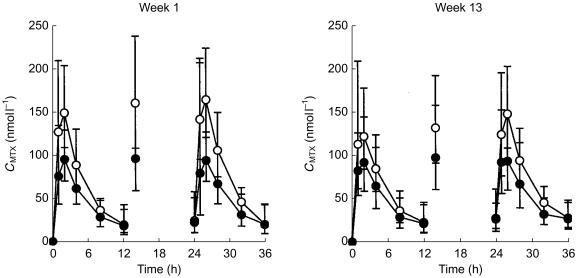
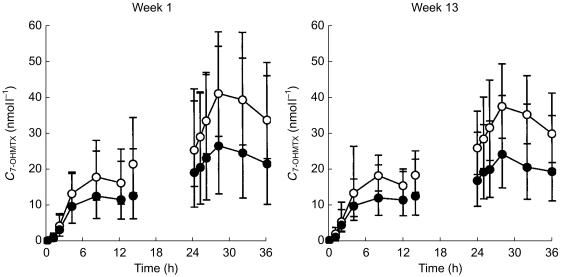
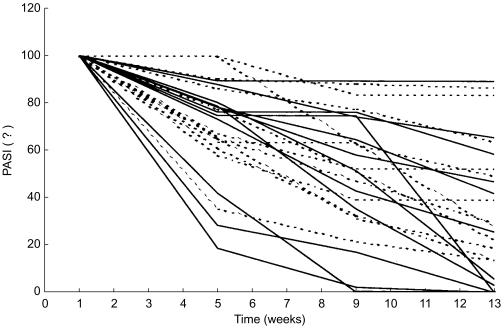
Methods: Twenty-four psoriatic patients (15 male and 9 female, aged 31-73 years) were given weekly doses of MTX doses of either 7.5 mg or 15 mg with each dose divided into three aliquots given at 12 h intervals. The pharmacokinetics of MTX were evaluated at weeks 1 and 13. Skin impairment was assessed using the PASI-scoring system (The Psoriasis Area and Severity Index) at baseline and at weeks 5, 9 and 13 of therapy. Haematological and biochemistry tests were also performed at these times.
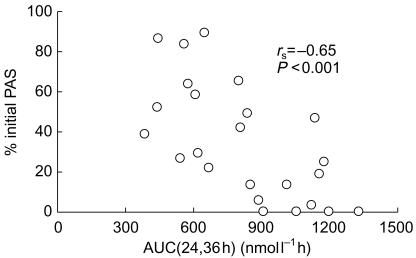
Results: The comparison of the areas under the plasma concentration-time curve (AUC(MTX)) after the first and third weekly doses showed that the extent of MTX accumulation in plasma was only about 12%. Two-way anova (factors: subject and the week of therapy) on the log-transformed AUC(MTX) showed no effect of the week of therapy (P>0.8). Moreover, the intraindividual variability in the AUC(MTX) was at least 4-fold less than the interindividual variability (F-test; P<0.01). The steady-state total plasma clearance of MTX ranged from 5.0 to 18.2 l h(-1) and was proportional to the renal clearance (r2=0.45, P<0.001) which accounted for 65+/-20% of the former. The renal clearance of 7-OHMTX was approximately 4-8% of that of the parent compound. PK/PD analysis revealed a highly significant inverse relationship between PASI (expressed as a percent of the initial value) and a steady-state AUC(MTX) (rs=-0.65, P<0.001). Seventeen subjects (8 from the 7.5 mg group and 9 from the 15 mg group MTX, P=0.67) achieved a greater than 50% decrease in the initial PASI score and were classified as responders. Thirteen of 14 subjects with AUC(24,36 h)> or =700 nmol l(-1) h responded to pharmacotherapy. Conversely, only 4 out of 10 subjects with AUC(24,36 h)<700 nmol l-1 h were responders (P<0.01, Fisher's exact test).
Conclusions: A strong correlation was observed between the pharmacokinetics (AUC(MTX) at the steady state) and antipsoriatic effect (PASI-score) of LDMTX. The considerable interindividual variability and low intraindividual variability in MTX pharmacokinetics support a role for therapeutic monitoring and dose individualization at the start of pharmacotherapy. The results of this study suggest that a steady state AUC(MTX) values of 700 nmol l(-1)h and higher are associated with a significantly better success rate of antipsoriatic therapy than lower values.
Figures
References
-
- Hendel J, Nyfors A. Non-linear renal elimination kinetics of methotrexate due to saturation of renal tubular reabsorption. Eur J Clin Pharmacol. 1984;26:121–124. - PubMed
-
- Van Dooren-Greebe JR, Kuipers ALA, Mulder JTh, De Boo Van de Kerkhof PCM. Methotrexate revisited. Effects of long-term treatment in psoriasis. Br J Dermatol. 1994;130:204–210. - PubMed
-
- Bannwarth B, Pehourcq F, Schaeverbeke T, Dehais J. Clinical pharmacokinetics of low-dose methotrexate in rheumatoid arthritis. Clin Pharmacokinet. 1996;30:194–210. - PubMed
-
- Songsiridej N, Furst DE. Methotrexate – the therapy rapidly acting drug. Baillieres Clin Rheumatol. 1990;4:575–593. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
