

Presenting risks and benefits to patients
- PMID: 12213142
- PMCID: PMC1495093
- DOI: 10.1046/j.1525-1497.2002.11001.x
Presenting risks and benefits to patients
Abstract
Objective: To investigate whether patients are influenced by the order in which they learn the risks and benefits of a treatment and whether this effect is attenuated by a treatment's associated risk and/or benefit.
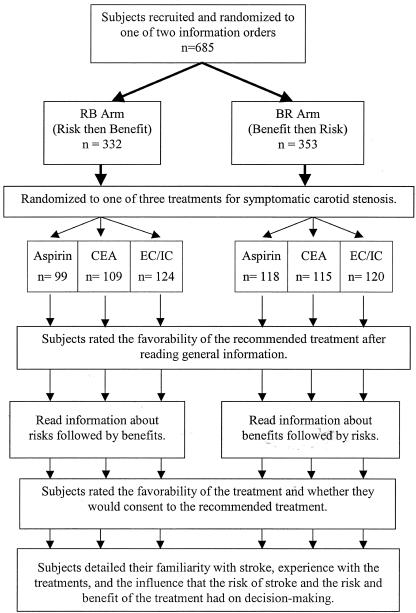
Design: Subjects were randomized to review 1 of 6 medical treatment information brochures.
Setting: Waiting rooms of primary care physicians at an academic health center.
Participants: Six hundred eighty-five subjects, ages 18 to 70 years.
Intervention: Subjects reviewed 1 of 3 treatments for symptomatic carotid artery disease. The first (aspirin) was low-risk/low-benefit, the second (carotid endarterectomy surgery) was high-risk/high-benefit, and the third (extracranial-to-intracranial bypass surgery) was high-risk but of unknown benefit. Patients were also randomized to receive information about risk either before or after benefit. Patients were asked to rate the favorability of the treatment on a scale of 0 to 100 and whether they would consent. Finally, subjects rated how their decisions were influenced by the risk and benefit information.
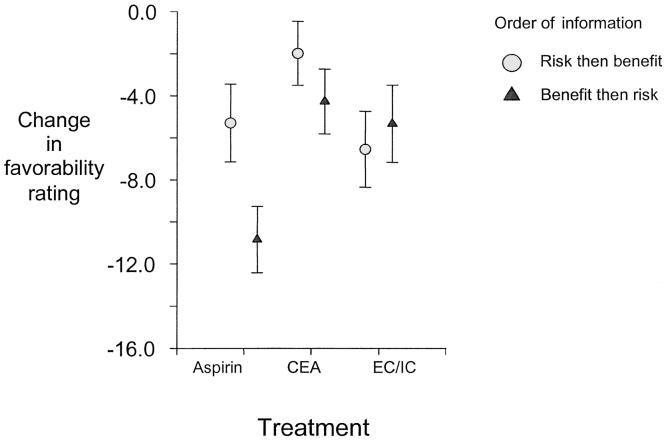
Main results: Subjects evaluating aspirin therapy were influenced by the order of the risk/benefit information. Those learning about risks after benefits had a greater drop in their favorability ratings than subjects learning about risks before benefits (-10.9 vs -5.2 on a 100-point scale; P = .02) and were less likely to consent (odds ratio, 2.27; P = .04). In contrast, subjects evaluating carotid endarterectomy and extracranial-to-intracranial bypass were not influenced by information order. When subjects were influenced by the order of information, they also reported that the treatment's risk had less influence on their decision making (P < .01).
Conclusions: When patients evaluate low-risk medical interventions, they may form less favorable impressions of the treatment and be less likely to consent to the treatment when they learn about the risks after the benefits. Order effects were not observed with high-risk treatments regardless of potential benefits.
Figures
References
-
- Hogarth RM, Einhorn HJ. Order effects in belief updating: the belief-adjustment model. Cognit Psychol. 1992;24:1–55.
-
- Strang KR, Schwei M, Geiselman RE. Effects of the structure of descriptions on group impression formation. Bull Psychosom Soc. 1978;12:224–26.
-
- Schadewald MS, Limberg ST. Effect of information order and accountability on causal judgments in a legal context. Psychol Rep. 1992;71:619–25.
-
- Adelman L, Bresnick T, Black PK, Marvin FF, Sak SG. Research with Patriot air defense officers—examining information order effects. Hum Factors. 1996;38:250–61.
-
- Tubbs RM, Gaeth GJ, Levin IP, VanOsdol LA. Order effects in belief updating with consistent and inconsistent evidence. J Behav Decis Making. 1993;6:257–69.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources