

Case Reports
doi: 10.1097/00008506-200210000-00003.
Cerebral injury predicted by transcranial Doppler ultrasonography but not electroencephalography during carotid endarterectomy
Affiliations
- PMID: 12357085
- PMCID: PMC2435244
- DOI: 10.1097/00008506-200210000-00003
Item in Clipboard
Case Reports
Cerebral injury predicted by transcranial Doppler ultrasonography but not electroencephalography during carotid endarterectomy
J Neurosurg Anesthesiol.
2002 Oct.
Abstract
When shunts are selectively used during carotid endarterectomy, the adequacy of collateral cerebral blood flow (CBF) after the carotid artery is clamped is determined by monitors based on different physiologic measurements. In this series of three patients, we used electroencephalography (EEG) to measure neuronal electrical activity and transcranial Doppler ultrasonography (TCD) to measure CBF velocity. In each of our cases, the EEG was unchanged from preclamp values, while TCD CBF velocity was dramatically reduced. All three patients had transient neuropsychometric or neurologic changes after surgery, which resolved.
Figures
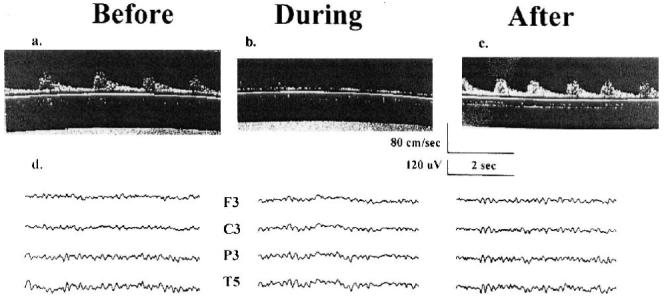
Transcranial Doppler ultrasonography and electroencephalogram. A, B and C are three transcranial Doppler (TCD) ultrasonography records from the patient reported in Case 1 with the TCD probe placed over the left temporal bone and insonated on the middle cerebral artery. “Before,” “during,” and “after” refer to three different records of cerebral blood flow (CBF) velocity taken at different times during surgery: before the carotid artery is clamped, while the carotid artery is clamped, and after the clamp has been removed. The scales for time in seconds and CBF velocity in cm/sec are shown below C. D shows three electroencephalographic (EEG) records taken at the three times described above. Ten electrodes are applied using an Electro-Cap (Electro-Cap International Inc., Eaton, OH). The electrodes are arranged in a referential montage using the International 10-20 positioning system with four over each hemisphere (Frontal [F], Central [C], Parietal [P], and Temporal [T]). The “reference” electrode placed centrally at Cz (“Z” refers to midline), and a “ground” electrode at Fz. Only the EEG traces for the left hemisphere are shown. The scales for time in seconds and EEG amplitude in μV are shown below C.
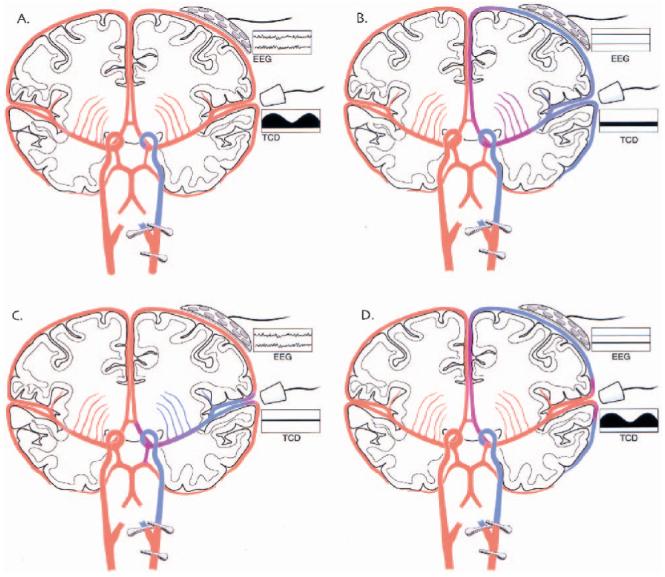
Coronal cross-section of the cerebral hemispheres showing: adequacy of cerebral perfusion, location of EEG and TCD monitors and their records. These four diagrams show coronal cross-sections of both cerebral hemispheres. The common carotid artery and its divisions have been clamped in all of the diagrams. The EEG and TCD monitors and their respective records are labeled. The adequacy of cerebral blood flow (CBF) after the carotid artery is clamped is color-coded. “Red” is CBF that is adequate to maintain normal neuronal functioning and “blue” is inadequate CBF for the same purpose. Shades of color between these two extremes are meant to illustrate a gradient of CBF. The EEG and TCD records are meant to depict “normal” EEG and TCD records in A and “abnormal” records in B. One record from each type of monitor is “normal” and “abnormal” in C and D. Cerebral blood flow velocity is abnormal in C and EEG, in D.
Similar articles
-
Continuous transcranial Doppler ultrasonography and electroencephalography during carotid endarterectomy: a multimodal monitoring system to detect intraoperative ischemia.Ann Vasc Surg. 1993 Jan;7(1):95-101. doi: 10.1007/BF02042666. Ann Vasc Surg. 1993. PMID: 8518125
-
[Multimodal neuromonitoring in the early diagnosis of brain ischemia during carotid arterial reconstruction].Anesteziol Reanimatol. 2008 Mar-Apr;(2):16-22. Anesteziol Reanimatol. 2008. PMID: 18540459 Russian.
-
Transcranial Doppler monitoring during carotid endarterectomy: a technical case report.J Neurosurg Anesthesiol. 2000 Jul;12(3):233-9. doi: 10.1097/00008506-200007000-00007. J Neurosurg Anesthesiol. 2000. PMID: 10905573 Free PMC article.
-
Intraoperative use of transcranial Doppler ultrasonography.Neurosurg Clin N Am. 1996 Oct;7(4):709-22. Neurosurg Clin N Am. 1996. PMID: 8905782 Review.
-
Transcranial Doppler ultrasonography in neurological surgery and neurocritical care.Neurosurg Focus. 2019 Dec 1;47(6):E2. doi: 10.3171/2019.9.FOCUS19611. Neurosurg Focus. 2019. PMID: 31786564 Review.
Cited by
-
Arterial blood pressure management during carotid endarterectomy and early cognitive dysfunction.Neurosurgery. 2014 Mar;74(3):245-51; discussion 251-3. doi: 10.1227/NEU.0000000000000256. Neurosurgery. 2014. PMID: 24335822 Free PMC article.
-
A pilot protocol and review of triple neuroprotection with targeted hypothermia, controlled induced hypertension, and barbiturate infusion during emergency carotid endarterectomy for acute stroke after failed tPA or beyond 24-hour window of opportunity.Ann Transl Med. 2020 Oct;8(19):1275. doi: 10.21037/atm-2020-cass-14. Ann Transl Med. 2020. PMID: 33178807 Free PMC article. Review.
References
-
- Moller JT, Cluitmans P, Rasmussen LS, et al. Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet. 1998;351:857–861. - PubMed
-
- Thal GD, Szabo MD, LopezBresnahan M, et al. Exacerbation or unmasking of focal neurologic deficits by sedatives. Anesthesiology. 1996;85:21–25. - PubMed
-
- Krul JM, van Gijn J, Ackerstaff RG, et al. Site and pathogenesis of infarcts associated with carotid endarterectomy. Stroke. 1989;20:324–328. - PubMed
-
- Rampil IJ, Holzer JA, Quest DO, et al. Prognostic value of computerized EEG analysis during carotid endarterectomy. Anesth Analg. 1983;62:186–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
