

Identification of chromosome 9 alterations and p53 accumulation in isolated carcinoma in situ of the urinary bladder versus carcinoma in situ associated with carcinoma
- PMID: 12368185
- PMCID: PMC1867272
- DOI: 10.1016/S0002-9440(10)64388-X
Identification of chromosome 9 alterations and p53 accumulation in isolated carcinoma in situ of the urinary bladder versus carcinoma in situ associated with carcinoma
Abstract
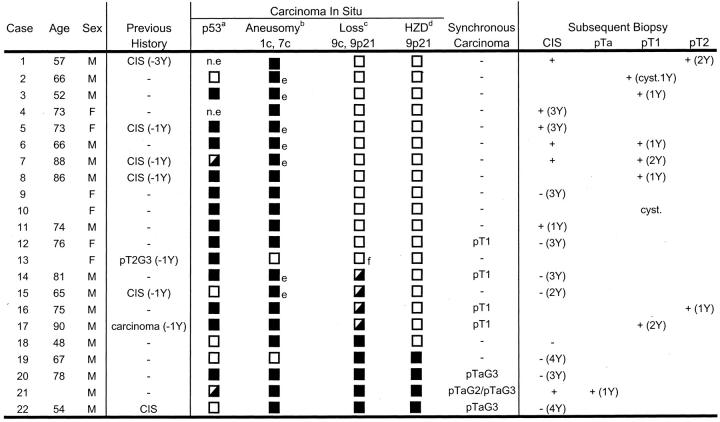
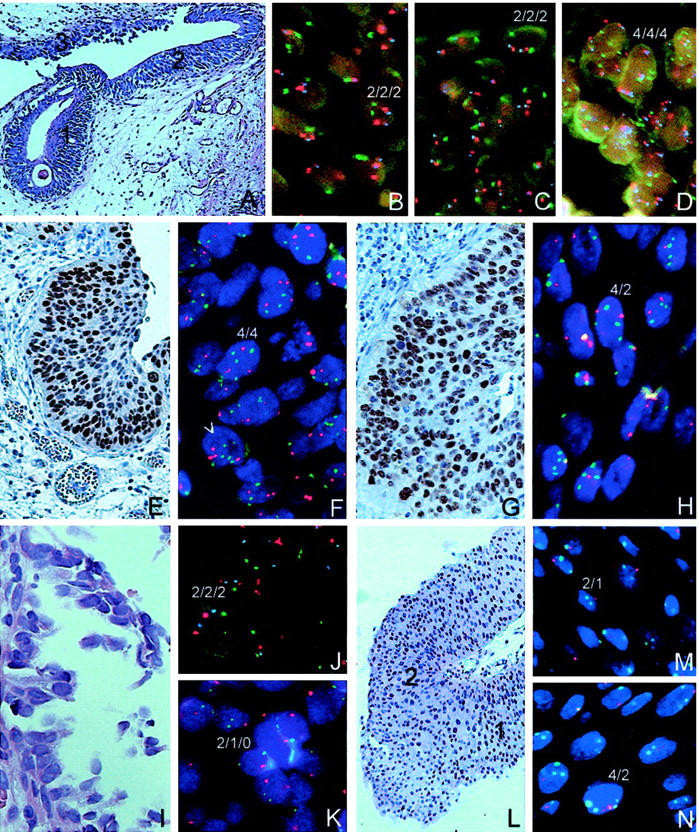
Carcinoma in situ (CIS) of the urinary bladder is a flat, aggressive lesion and may be the most common precursor of invasive bladder cancer. Although chromosome 9 alterations are among the earliest and most prevalent genetic alterations in bladder cancer, discrepancy exists about the frequency of chromosome 9 losses in CIS. We analyzed 22 patients with CIS of the bladder (15 patients with isolated CIS, 7 patients combined with synchronous pTa or pT1 carcinomas) for gains and losses of chromosome (peri)centromere loci 1q12, 7p11-q11, 9p11-q12, and 9p21 harboring the INK4A/ARF locus (p16(INK4A)/p14(ARF)) and INK4B (p15(INK4B)) by multiple-target fluorescence in situ hybridization, and for p53 protein accumulation by immunohistochemistry. In 15 of 20 (75%) CIS lesions analyzed p53 overexpression was detected, whereas aneusomy for chromosomes 1 and 7 was identified in 20 of 22 (91%) CIS. In 13 of 22 (60%) CIS cases analyzed, 12 of which were not associated with a synchronous pTa or pT1 carcinoma, no numerical losses for chromosome 9 (p11-q12 and 9p21) were detected as compared with chromosomes 1 and 7. Furthermore 6 of 12 (50%) patients showed a metachronous invasive carcinoma within 2 years. In the remaining nine biopsies CIS lesions (40%) were recognized that showed losses of chromosome 9p11-q12 and 9p21, six of these were associated with a synchronous pTa or pT1 carcinoma. Three of these carcinomas were pTa and exhibited loss of 9q12 as well as a homozygous deletion of 9p21. The others were invasive carcinomas in which CIS lesions were also recognized that showed no numerical loss of chromosome 9, but did show an accumulation of p53. In conclusion our data demonstrate that predominantly isolated CIS lesions contained cells with no specific loss of chromosome 9, as opposed to CIS lesions with synchronous carcinomas that showed evidence of chromosome 9 loss. Furthermore our data strengthen the proposition that p53 mutations (p53 overexpression) precede loss of chromosomes 9 and 9p21 in CIS as precursor for invasive bladder cancer, as opposed to noninvasive carcinomas where chromosome 9 (9p11-q12) losses are early and frequently combined with homozygous deletions of 9p21.
Figures

References
-
- Koss LG: Mapping of the urinary bladder: its impact on the concepts of bladder cancer. Hum Pathol 1979, 10:533-548 - PubMed
-
- Amin MB, Young RH: Intraepithelial lesions of the urinary bladder with a discussion of the histogenesis of urothelial neoplasia. Semin Surg Oncol 1997, 14:84-97 - PubMed
-
- Epstein JI, Amin MB, Reuter VR, Mostofi FK: The World Health Organization/International Society of Urological Pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder. Am J Surg Pathol 1998, 22:1435-1448 - PubMed
-
- Jones PA, Droller MJ: Pathways of development and progression in bladder cancer: new correlations between clinical observations and molecular mechanisms. Semin Urol 1993, 4:177-192 - PubMed
-
- Cordon-Cardo C: Molecular alterations in bladder cancer. Cancer Surv 1998, 32:115-131 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
