

Improvement in perioperative outcome after hepatic resection: analysis of 1,803 consecutive cases over the past decade
- PMID: 12368667
- PMCID: PMC1422593
- DOI: 10.1097/01.SLA.0000029003.66466.B3
Improvement in perioperative outcome after hepatic resection: analysis of 1,803 consecutive cases over the past decade
Abstract
Objective: To assess the nature of changes in the field of hepatic resectional surgery and their impact on perioperative outcome.
Methods: Demographics, extent of resection, concomitant major procedures, operative and transfusion data, complications, and hospital stay were analyzed for 1,803 consecutive patients undergoing hepatic resection from December 1991 to September 2001 at Memorial Sloan-Kettering Cancer Center. Factors associated with morbidity and mortality and trends in operative and perioperative variables over the period of study were analyzed.
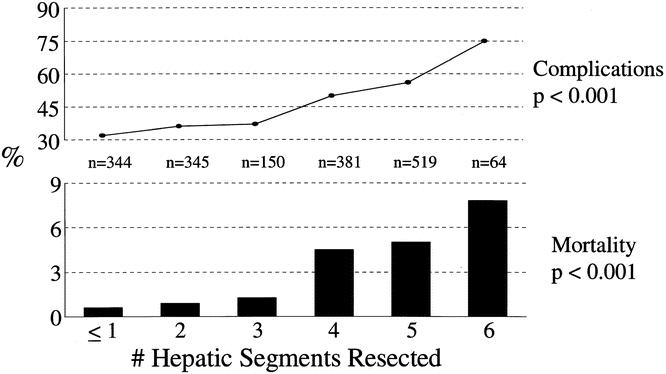
Results: Malignant disease was the most common diagnosis (1,642 patients, 91%); of these cases, metastatic colorectal cancer accounted for 62% (n = 1,021). Three hundred seventy-five resections (21%) were performed for primary hepatic or biliary cancers and 161 (9%) for benign disease. Anatomical resections were performed in 1,568 patients (87%) and included 544 extended hepatectomies, 483 hepatectomies, and 526 segmental resections. Sixty-two percent of patients had three or more segments resected, 42% had bilobar resections, and 37% had concomitant additional major procedures. The median blood loss was 600 mL and 49% of patients were transfused at any time during the index admission. Median hospital stay was 8 days, morbidity was 45%, and operative mortality was 3.1%. Over the study period, there was a significant increase in the use of parenchymal-sparing segmental resections and a decrease in the number of hepatic segments resected. In parallel with this, there was a significant decline in blood loss, the use of blood products, and hospital stay. Despite an increase in concomitant major procedures, operative mortality decreased from approximately 4% in the first 5 years of the study to 1.3% in the last 2 years, with 0 operative deaths in the last 184 consecutive cases. On multivariate analysis, the number of hepatic segments resected and operative blood loss were the only independent predictors of both perioperative morbidity and mortality.
Conclusions: Over the past decade, the use of parenchymal-sparing segmental resections has increased significantly. The number of hepatic segments resected and operative blood loss were the only predictors of both perioperative morbidity and mortality, and reductions in both are largely responsible for the decrease in perioperative mortality, which has occurred despite an increase in concomitant major procedures.
Figures

Comment in
-
Hepatic surgery: current techniques and outcomes.Curr Surg. 2005 Jul-Aug;62(4):374-82. doi: 10.1016/j.cursur.2004.09.009. Curr Surg. 2005. PMID: 15964458 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
